

Delta inflation: a bias in the design of randomized controlled trials in critical care medicine
- PMID: 20429873
- PMCID: PMC2887200
- DOI: 10.1186/cc8990
Delta inflation: a bias in the design of randomized controlled trials in critical care medicine
Abstract
Introduction: Mortality is the most widely accepted outcome measure in randomized controlled trials of therapies for critically ill adults, but most of these trials fail to show a statistically significant mortality benefit. The reasons for this are unknown.
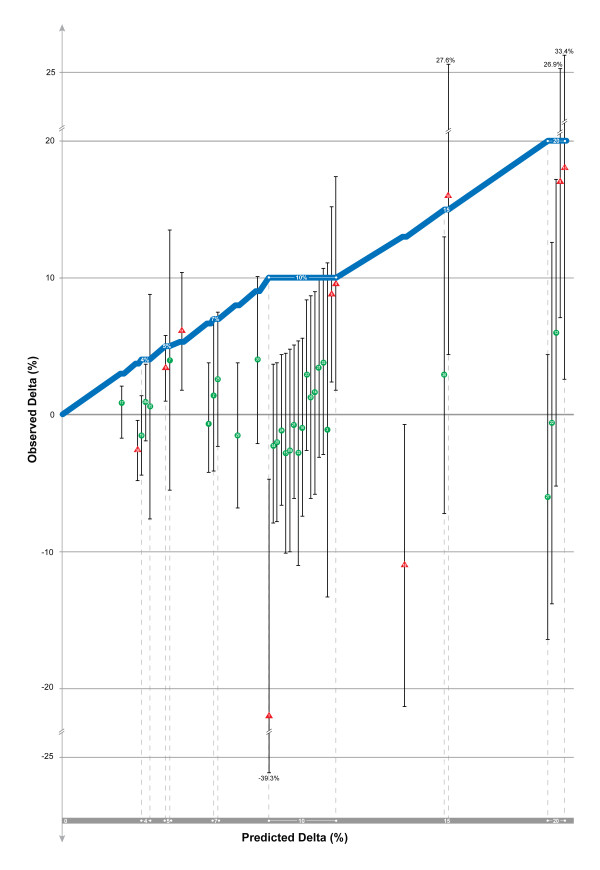
Methods: We searched five high impact journals (Annals of Internal Medicine, British Medical Journal, JAMA, The Lancet, New England Journal of Medicine) for randomized controlled trials comparing mortality of therapies for critically ill adults over a ten year period. We abstracted data on the statistical design and results of these trials to compare the predicted delta (delta; the effect size of the therapy compared to control expressed as an absolute mortality reduction) to the observed delta to determine if there is a systematic overestimation of predicted delta that might explain the high prevalence of negative results in these trials.
Results: We found 38 trials meeting our inclusion criteria. Only 5/38 (13.2%) of the trials provided justification for the predicted delta. The mean predicted delta among the 38 trials was 10.1% and the mean observed delta was 1.4% (P < 0.0001), resulting in a delta-gap of 8.7%. In only 2/38 (5.3%) of the trials did the observed delta exceed the predicted delta and only 7/38 (18.4%) of the trials demonstrated statistically significant results in the hypothesized direction; these trials had smaller delta-gaps than the remainder of the trials (delta-gap 0.9% versus 10.5%; P < 0.0001). For trials showing non-significant trends toward benefit greater than 3%, large increases in sample size (380% - 1100%) would be required if repeat trials use the observed delta from the index trial as the predicted delta for a follow-up study.
Conclusions: Investigators of therapies for critical illness systematically overestimate treatment effect size (delta) during the design of randomized controlled trials. This bias, which we refer to as "delta inflation", is a potential reason that these trials have a high rate of negative results."Absence of evidence is not evidence of absence."
Figures
Comment in
-
Underpowered trials in critical care medicine: how to deal with them?Crit Care. 2010;14(3):423. doi: 10.1186/cc9021. Epub 2010 Jun 8. Crit Care. 2010. PMID: 20553632 Free PMC article. No abstract available.
References
-
- Annane D, Sébille V, Charpentier C, Bollaert PE, François B, Korach JM, Capellier G, Cohen Y, Azoulay E, Troché G, Chaumet-Riffaud P, Bellissant E. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA. 2002;288:862–871. doi: 10.1001/jama.288.7.862. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
