

Long-term cancer risk of immunosuppressive regimens after kidney transplantation
- PMID: 20431040
- PMCID: PMC2865745
- DOI: 10.1681/ASN.2009101043
Long-term cancer risk of immunosuppressive regimens after kidney transplantation
Abstract
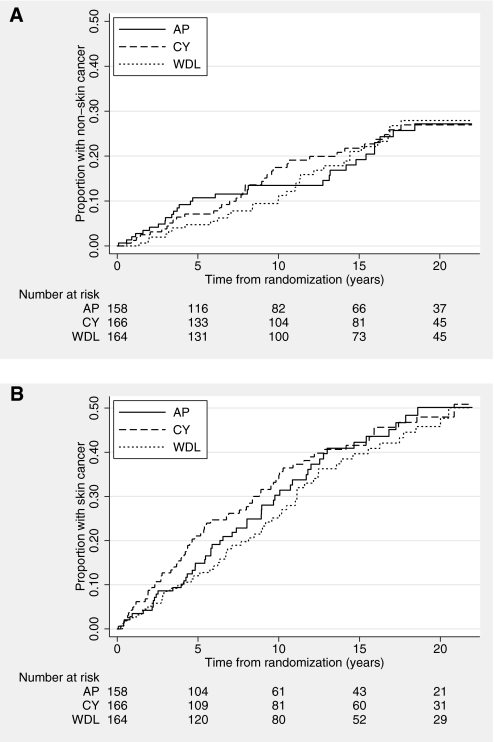
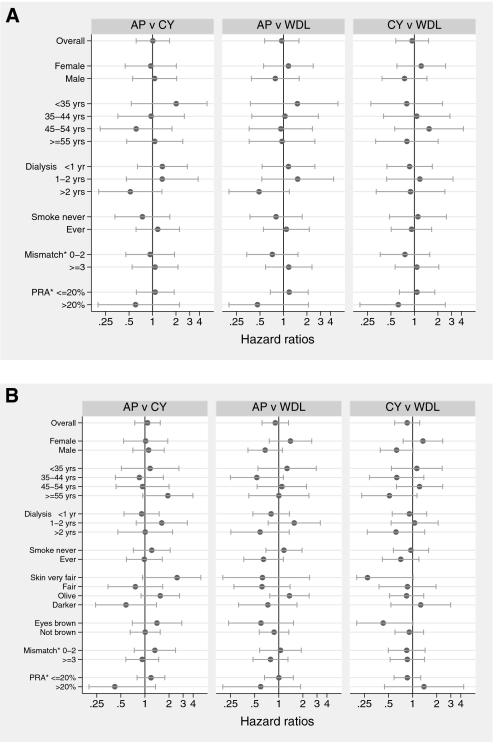
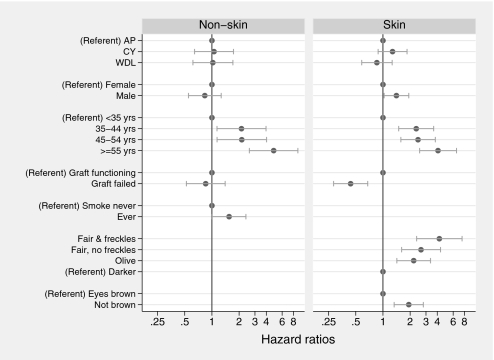
Cancer is a widely recognized complication of transplantation, and the effects of various immunosuppressive drugs on cancer risk remains controversial. This randomized trial allocated 489 recipients of first cadaveric renal transplants to one of three groups: Azathioprine and prednisolone, cyclosporine monotherapy, or cyclosporine monotherapy followed by a switch to azathioprine and prednisolone after 3 months. Here, we report cancer outcomes by non-skin cancer (including melanoma) and skin cancer (excluding melanoma) for 481 patients during a median follow-up of 20.6 years. A total of 226 patients developed at least one cancer: 95 with non-skin cancer and 171 with skin cancer. In the intention-to-treat analysis, mean times to first non-skin cancer (16.0, 15.3, and 15.7 years for groups 1 through 3, respectively) and first skin cancer (13.6, 14.3, and 15.2 years, respectively) were not different among the three groups or between any subgroup. In multivariate analyses, non-skin cancer associated with increasing age and previous smoking history, whereas skin cancer associated with increasing age, nonbrown eye color, fairer skin, and a functioning transplant. Treatment allocation did not associate with development of either form of cancer in multivariate analyses. In conclusion, these immunosuppressive regimens, widely used in recent decades, carry similar risks for carcinogenicity after kidney transplantation.
Figures
References
-
- Vajdic CM, McDonald SP, McCredie MR, van Leeuwen MT, Stewart JH, Law M, Chapman JR, Webster AC, Kaldor JM, Grulich AE: Cancer incidence before and after kidney transplantation. JAMA 296: 2823–2831, 2006. - PubMed
-
- Birkeland SA, Storm HH, Lamm LU, Barlow L, Blohme I, Forsberg B, Eklund B, Fjeldborg O, Friedberg M, Frödin L, et al. : Cancer risk after renal transplantation in the Nordic countries, 1964–1986. Int J Cancer 60: 183–189, 1995. - PubMed
-
- Webster AC, Craig JC, Simpson JM, Jones MP, Chapman JR: Identifying high risk groups and quantifying absolute risk of cancer after kidney transplantation: A cohort study of 15,183 recipients. Am J Transplant 7: 2140–2151, 2007. - PubMed
-
- Gallagher M, Jardine M, Perkovic V, Cass A, McDonald S, Petrie J, Eris J: Cyclosporine withdrawal improves long-term graft survival in renal transplantation. Transplantation 87: 1877–1883, 2009. - PubMed
-
- Gallagher MP, Hall B, Craig J, Berry G, Tiller DJ, Eris J: A randomized controlled trial of cyclosporine withdrawal in renal-transplant recipients: 15-Year results. Transplantation 78: 1653–1660, 2004. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
