

Induction and maintenance of therapeutic hypothermia after pediatric cardiac arrest: efficacy of a surface cooling protocol
- PMID: 20431502
- PMCID: PMC3740551
- DOI: 10.1097/PCC.0b013e3181e28717
Induction and maintenance of therapeutic hypothermia after pediatric cardiac arrest: efficacy of a surface cooling protocol
Abstract
Objective: To assess the feasibility, effectiveness, side effects, and adverse events associated with a standardized surface cooling protocol. Induced therapeutic hypothermia after pediatric cardiac arrest is an important intervention.
Design: Prospective intervention trial.
Setting: Urban, tertiary care children's hospital.
Patients: Twelve pediatric cardiac arrest survivors.
Interventions: Standardized surface cooling protocol.
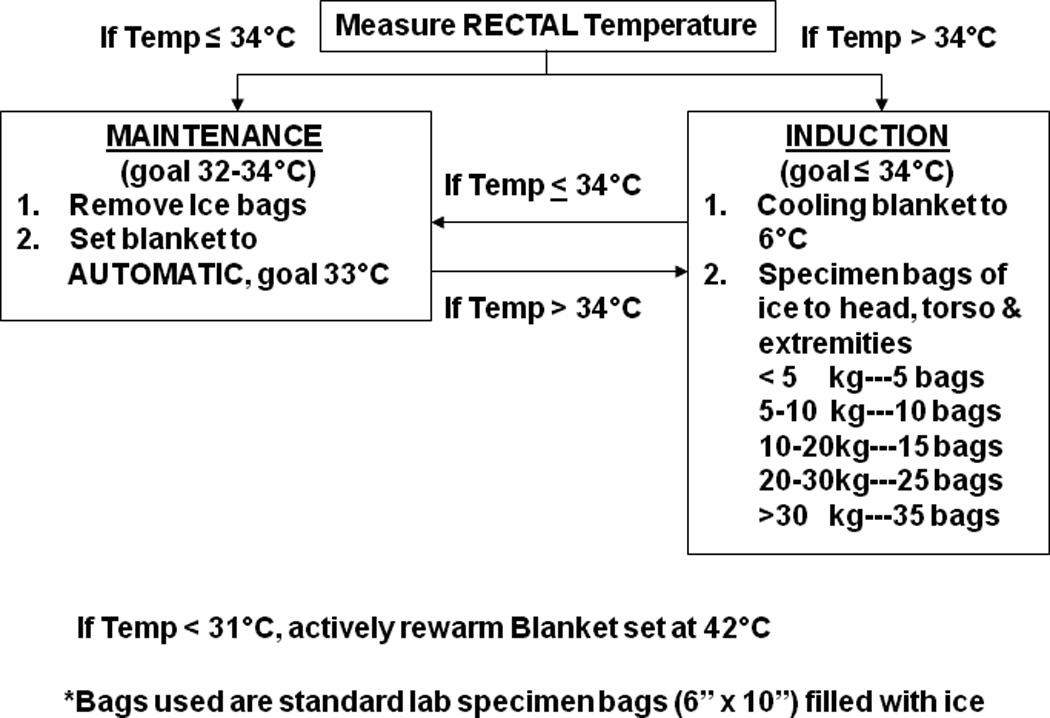
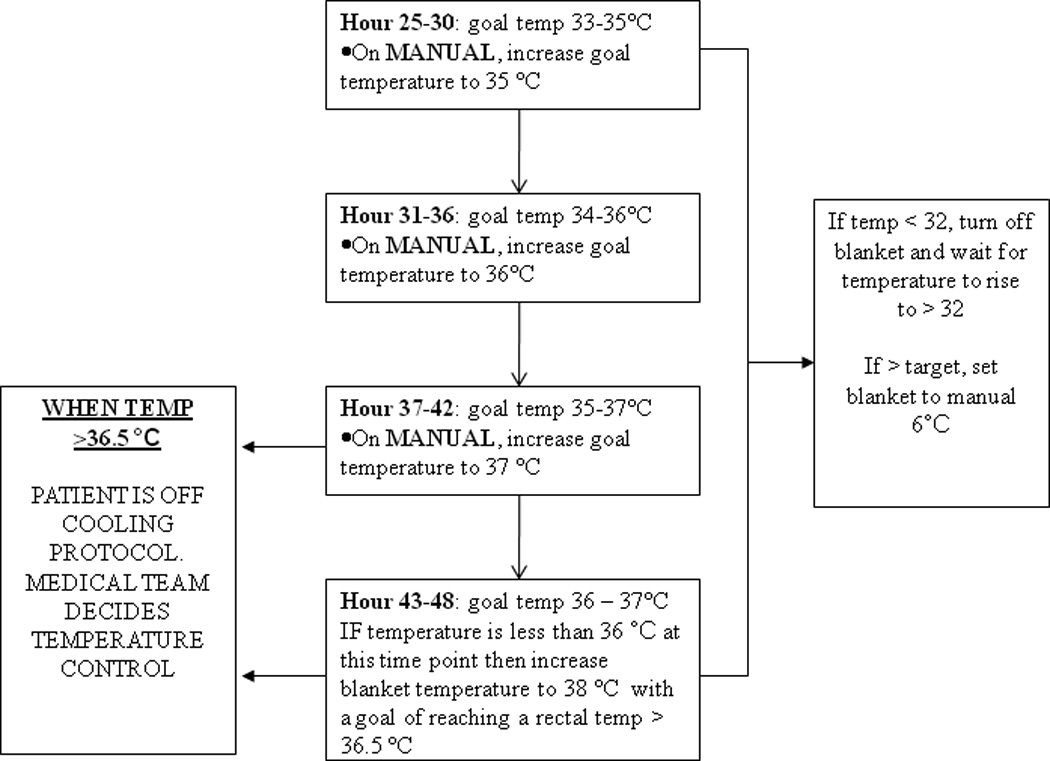
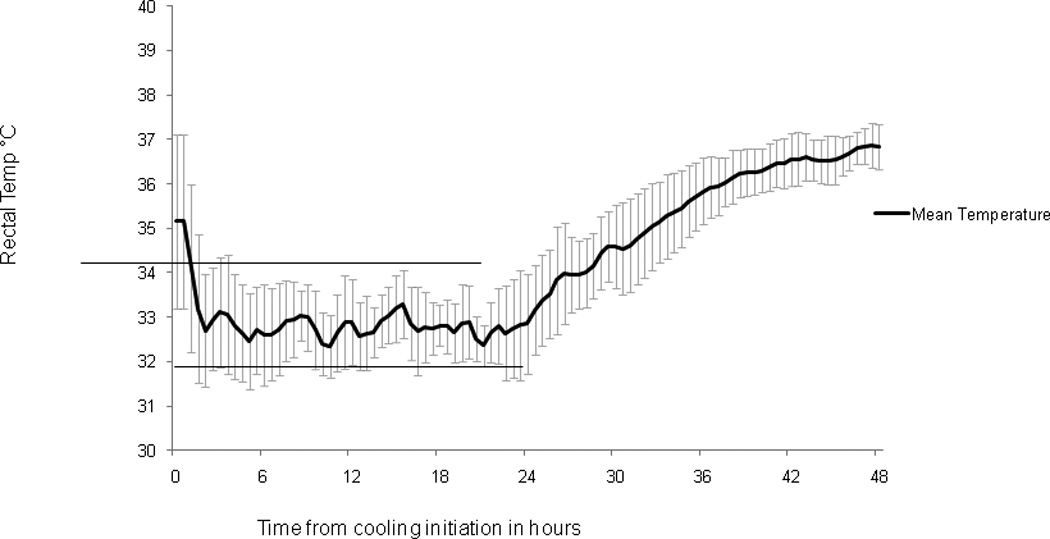
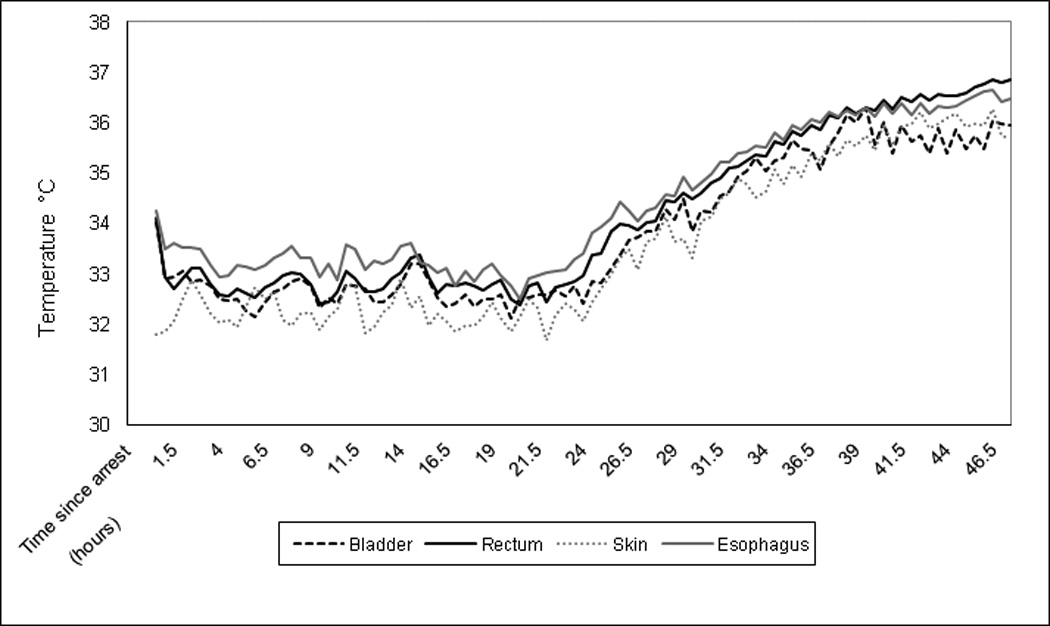
Measurements and main results: Patients (age: median, 1.5 yrs; interquartile range, 0.5-6.25; cardiopulmonary resuscitation duration: median, 18 mins; interquartile range, 10-45) were cooled by a standard surface cooling protocol for rapid induction and maintenance of goal rectal temperature (T) 32°C-34°C for 24 hrs, with prospectively defined rescue protocols. Side effects and clinical interventions were recorded. Median time to rectal T ≤34°C was 1.5 (1, 1.5) hrs from cooling initiation and 6 (5, 6.5) hrs from arrest. T was documented every 30 mins. Maintenance target T 32°C-34°C was attained in 78% (414 of 531) of measurements, overshoot hypothermia <32°C in 15% (81 of 531), and overshoot hyperthermia >34°C in 7% (36 of 531). Mean bias between rectal vs. esophageal T was -0.42°C (95% confidence interval, -0.49 to -0.35), and between rectal and bladder T was 0.16°C (95% confidence interval, 0.11-0.22). Side effects observed included: hypokalemia <3.0 mEq/L in 67% of patients and bradycardia <2% for age in 58%. There were no episodes of bleeding or ventricular tachyarrhythmia that required treatment. Six (50%) of 12 patients survived to discharge.
Conclusions: A standard surface cooling protocol achieved rapid induction of hypothermia after pediatric cardiac arrest. During maintenance of hypothermia, 78% of measures were within target T 32°C-34°C. Commonly employed temperature sites (esophageal, rectal, and bladder) were similar. Overshoot hypothermia and associated side effects were common, but there were no serious adverse events attributable to induced therapeutic hypothermia in this case series. Surface cooling protocols to induce and maintain therapeutic hypothermia after pediatric cardiac arrest are potentially feasible.
Conflict of interest statement
Conflicts of Interest: Alexis Topjian, Rebecca Ichord and Vinay Nadkarni each receive NHLBI funding as investigators for the Therapeutic Hypothermia After Cardiac Arrest study.
Figures
Comment in
-
Therapeutic hypothermia: ready...fire...aim? How small feasibility studies can inform large efficacy trials.Pediatr Crit Care Med. 2011 May;12(3):370-1. doi: 10.1097/PCC.0b013e3181e8b7ef. Pediatr Crit Care Med. 2011. PMID: 21637154 No abstract available.
References
-
- Nadkarni VM, Larkin GL, Peberdy MA, et al. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. Jama. 2006;295:50–57. - PubMed
-
- Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–563. - PubMed
-
- Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549–556. - PubMed
-
- 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2005;112:IV1–IV203. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
