

Malignant tumours of the kidney: imaging strategy
- PMID: 20432020
- PMCID: PMC2861760
- DOI: 10.1007/s00247-010-1584-z
Malignant tumours of the kidney: imaging strategy
Abstract
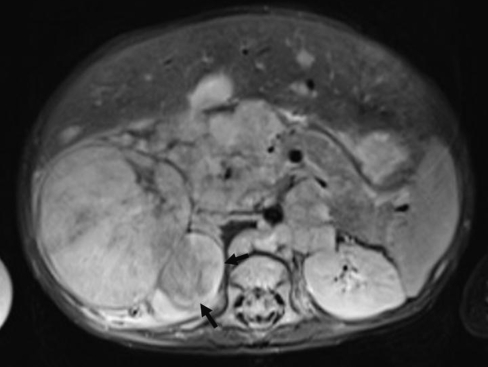
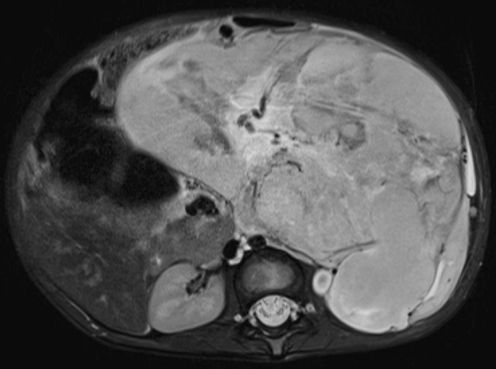
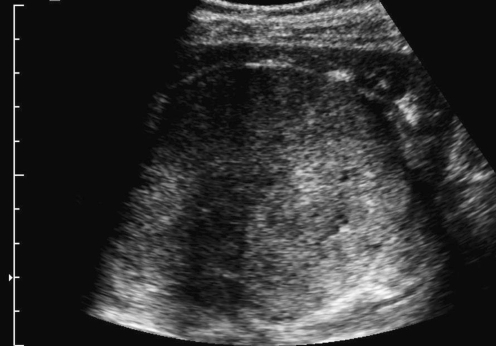
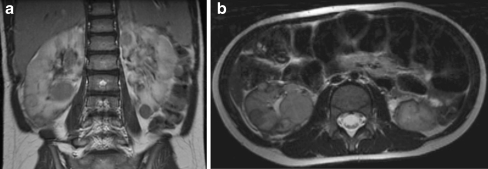
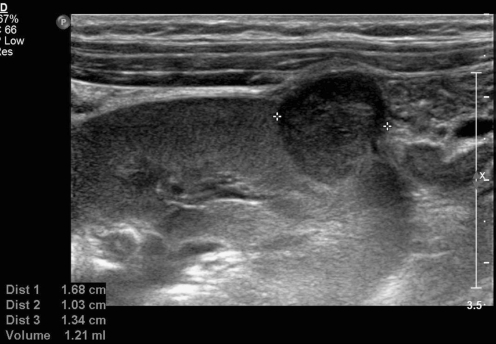
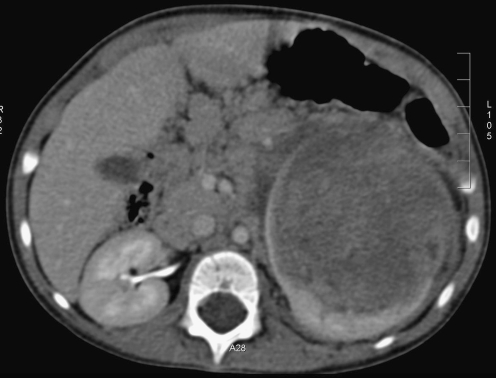
Primitive malignant renal tumours comprise 6% of all childhood cancers. Wilms tumour (WT) or nephroblastoma is the most frequent type accounting for more than 90%. Imaging alone cannot differentiate between these tumours with certainty but it plays an important role in screening, diagnostic workup, assessment of therapy response, preoperative evaluation and follow-up. The outcome of WT after therapy is excellent with an overall survival around 90%. In tumours such as those where the outcome is extremely good, focus can be shifted to a risk-based stratification to maintain excellent outcome in children with low risk tumours while improving quality of life and decreasing toxicity and costs. This review will discuss the imaging issues for WT from the European perspective and briefly discuss the characteristics of other malignant renal tumours occurring in children and new imaging techniques with potential in this matter.
Figures


References
-
- SIOP (2001) Nephroblastoma clinical trial and study protocol. In: Oncology ISoP (ed), pp 1–170
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
