

The persistent problem of new-onset postoperative atrial fibrillation: a single-institution experience over two decades
- PMID: 20434173
- PMCID: PMC2917532
- DOI: 10.1016/j.jtcvs.2010.03.011
The persistent problem of new-onset postoperative atrial fibrillation: a single-institution experience over two decades
Abstract
Objective: Postoperative atrial fibrillation is the most common complication after cardiac surgery. A variety of postoperative atrial fibrillation risk factors have been reported, but study results have been inconsistent or contradictory, particularly in patients with preexisting atrial fibrillation. The incidence of postoperative atrial fibrillation was evaluated in a group of 10,390 patients undergoing cardiac surgery among a comprehensive range of risk factors to identify reliable predictors of postoperative atrial fibrillation.
Methods: This 20-year retrospective study examined the relationship between postoperative atrial fibrillation and demographic factors, preoperative health conditions and medications, operative procedures, and postoperative complications. Multivariate logistic regression models were used to evaluate potential predictors of postoperative atrial fibrillation.
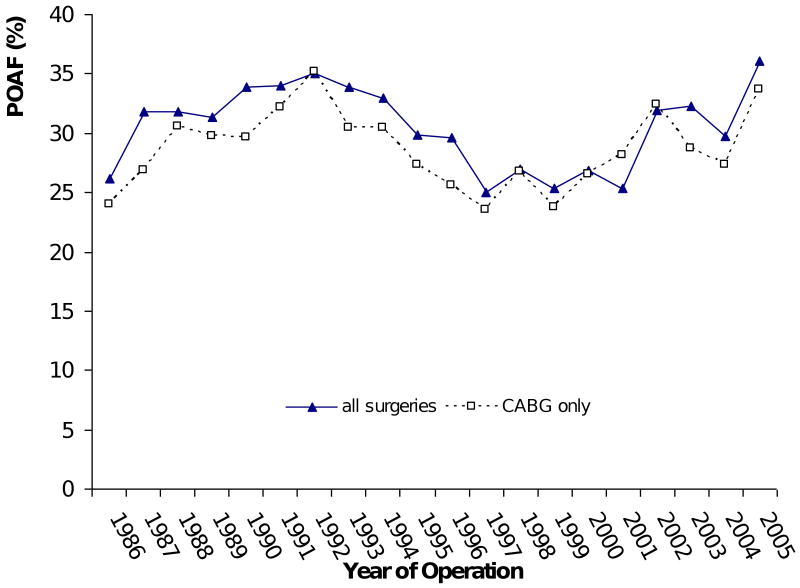
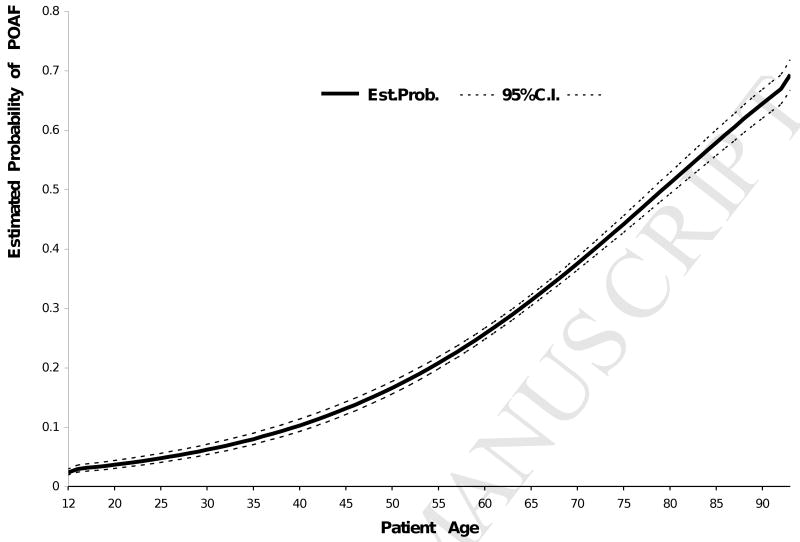
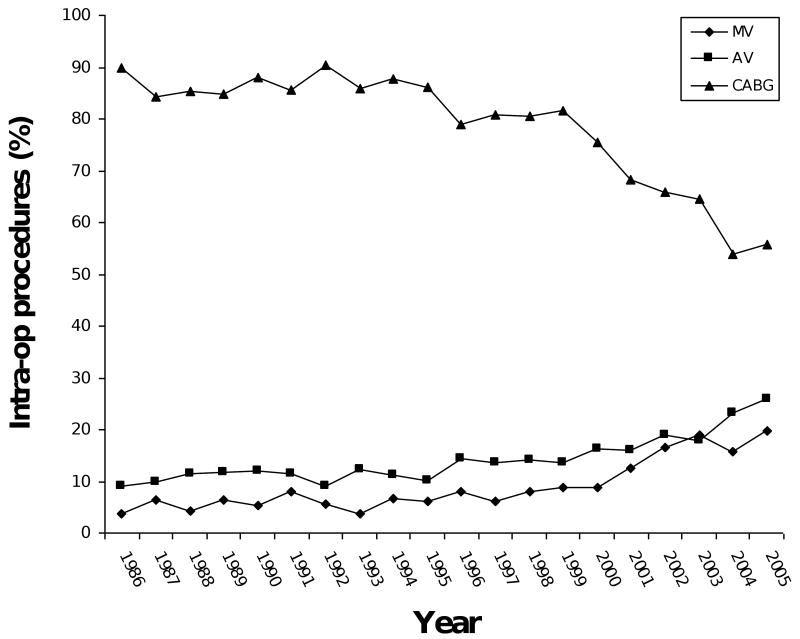
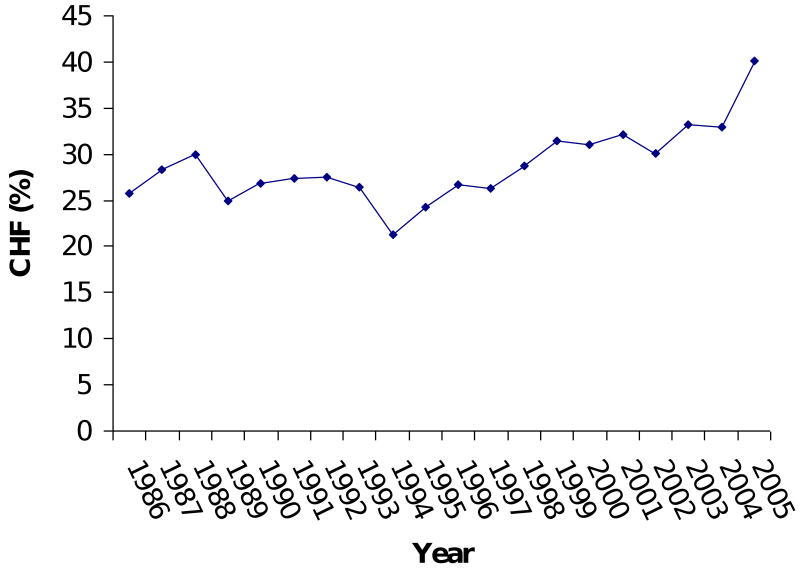
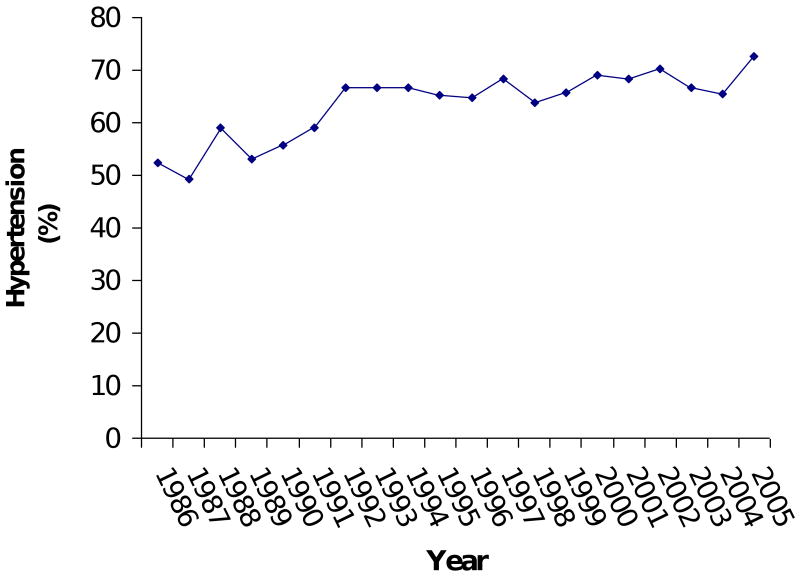
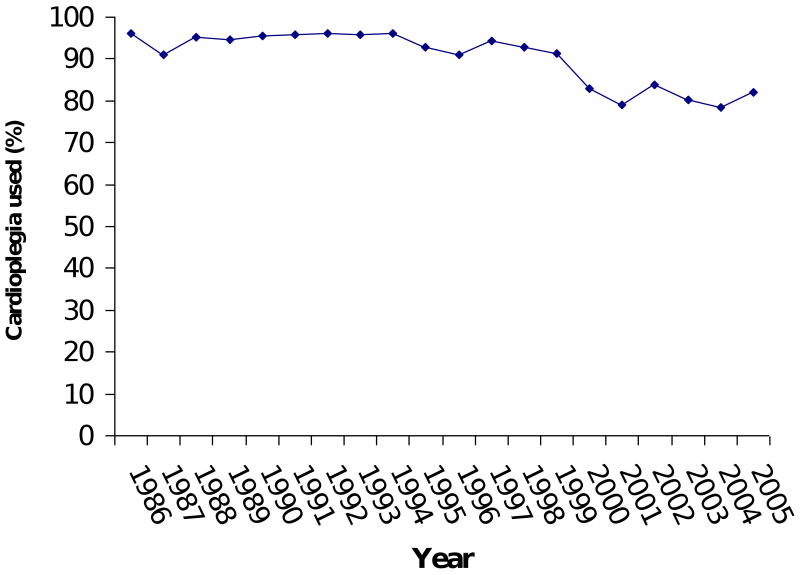
Results: Increasing age, mitral valve surgery (odds ratio=1.91), left ventricular aneurysm repair (odds ratio=1.57), aortic valve surgery (odds ratio=1.52), race (Caucasian) (odds ratio=1.51), use of cardioplegia (odds ratio=1.36), use of an intraaortic balloon pump (odds ratio=1.28), previous congestive heart failure (odds ratio=1.28), and hypertension (odds ratio=1.15) were significantly associated with postoperative atrial fibrillation. The non-linear relationship between age and postoperative atrial fibrillation revealed the acceleration of postoperative atrial fibrillation risk in patients aged 55 years or more. In patients undergoing coronary artery bypass grafting, increasing age and previous congestive heart failure were the only factors associated with a higher risk of postoperative atrial fibrillation. There was no trend in incidence of postoperative atrial fibrillation over time. No protective factors against postoperative atrial fibrillation were detected, including commonly prescribed categories of medications.
Conclusions: The persistence of the problem of postoperative atrial fibrillation and the modest predictability using common risk factors suggest that limited progress has been made in understanding its cause and treatment.
Copyright © 2011 The American Association for Thoracic Surgery. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Ommen SR, Odell JA, Stanton MS. Atrial arrhythmias after cardiothoracic surgery. N Engl J Med. 1997;336(20):1429–34. - PubMed
-
- Creswell LL, Schuessler RB, Rosenbloom M, Cox JL. Hazards of postoperative atrial arrhythmias. Ann Thorac Surg. 1993;56:539–49. - PubMed
-
- Aranki SF, Shaw DP, Adams DH, Rizzo RJ, Couper GS, VanderVliet M, et al. Predictors of atrial fibrillation after coronary artery surgery: current trends and impact on hospital resources. Circulation. 1996;94:390–7. - PubMed
-
- Hashimoto K, Ilstrup DM, Schaff HV. Influence of clinical and hemodynamic variables on risk of supraventricular tachycardia after coronary artery bypass. J Thorac Cardiovasc Surg. 1991;101:56–65. - PubMed
-
- Leitch JW, Thomson D, Baird Dk, Harris PJ. The importance of age as a predictor of artial fibrillation and flutter after coronary artery bypass grafting. J Thorac Cardiovasc Surg. 1990;100:338–42. - PubMed
