

Independent predictors of survival in primary systemic (Al) amyloidosis, including cardiac biomarkers and left ventricular strain imaging: an observational cohort study
- PMID: 20434879
- PMCID: PMC4041492
- DOI: 10.1016/j.echo.2010.03.027
Independent predictors of survival in primary systemic (Al) amyloidosis, including cardiac biomarkers and left ventricular strain imaging: an observational cohort study
Abstract
Background: The prognostic value of Doppler myocardial imaging, including myocardial velocity imaging, strain, and strain rate imaging, in patients with primary (AL) amyloidosis is uncertain. The aim of this longitudinal study was to identify independent predictors of survival, comparing clinical data, hematologic and cardiac biomarkers, and standard echocardiographic and Doppler myocardial imaging measures in a cohort of patients with AL amyloidosis.
Methods: A total of 249 consecutive patients with AL amyloidosis were prospectively enrolled. The primary end point was all-cause mortality, and during a median follow-up period of 18 months, 75 patients (30%) died. Clinical and electrocardiographic data, biomarkers (brain natriuretic peptide and cardiac troponin T) and standard echocardiographic and longitudinal systolic and diastolic Doppler myocardial imaging measurements for 16 left ventricular segments were tested as potential independent predictors of survival.
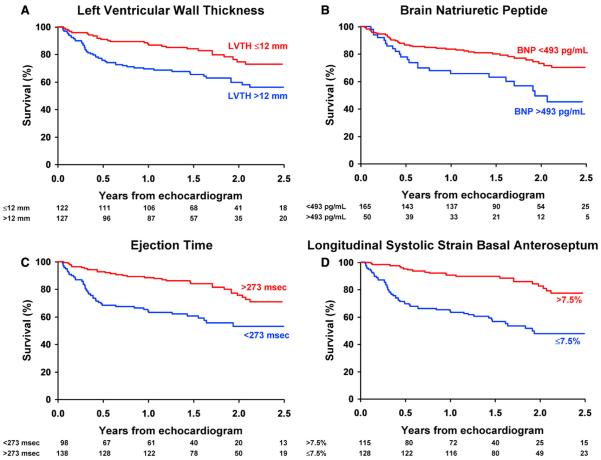
Results: Age (hazard ratio [HR], 1.03; P = .03), New York Heart Association class III or IV (HR, 2.47; P = .01), the presence of pleural effusion (HR, 1.79; P = .08), brain natriuretic peptide level (HR, 1.29; P = .01), ejection time (HR, 0.99; P = .13), and peak longitudinal systolic strain of the basal anteroseptal segment (HR, 1.05; P = .02) were independent predictors in the final model.
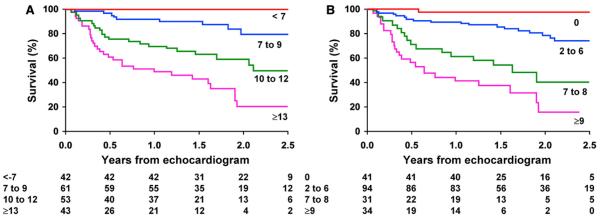
Conclusions: Multivariate survival analysis identified independent predictors of clinical outcome in patients with AL amyloidosis: New York Heart Association class III or IV, presence of pleural effusion, brain natriuretic peptide level > 493 pg/mL, ejection time < 273 ms, and peak longitudinal systolic basal anteroseptal strain less negative than or equal to -7.5% defined a high-risk group of patients.
Copyright 2010 American Society of Echocardiography. Published by Mosby, Inc. All rights reserved.
Figures
Comment in
-
Light chain amyloidosis circa 2010: six prognostic markers and one sobering reality.J Am Soc Echocardiogr. 2010 Jun;23(6):653-5. doi: 10.1016/j.echo.2010.04.008. J Am Soc Echocardiogr. 2010. PMID: 20497862 No abstract available.
References
-
- Wright JR, Calkins E. Clinical-pathologic differentiation of common amyloid syndromes. Medicine (Baltimore) 1981;60:429–48. - PubMed
-
- Dispenzieri A, Gertz MA, Kyle RA, Lacy MQ, Burritt MF, Therneau TM, et al. Prognostication of survival using cardiac troponins and N-terminal pro-brain natriuretic peptide in patients with primary systemic amyloidosis undergoing peripheral blood stem cell transplantation. Blood. 2004;104:1881–7. - PubMed
-
- Koyama J, Ray-Sequin PA, Falk RH. Longitudinal myocardial function assessed by tissue velocity, strain, and strain rate tissue Doppler echocardiography in patients with AL (primary) cardiac amyloidosis. Circulation. 2003;107:2446–52. - PubMed
-
- Bellavia D, Pellikka PA, Abraham TP, Al-Zahrani GB, Dispenzieri A, Oh JK, et al. Evidence of impaired left ventricular systolic function by Doppler myocardial imaging in patients with systemic amyloidosis and no evidence of cardiac involvement by standard two-dimensional and Doppler echocardiography. Am J Cardiol. 2008;101:1039–45. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
