

The influence of torsion on disc herniation when combined with flexion
- PMID: 20437184
- PMCID: PMC2989279
- DOI: 10.1007/s00586-010-1383-0
The influence of torsion on disc herniation when combined with flexion
Abstract
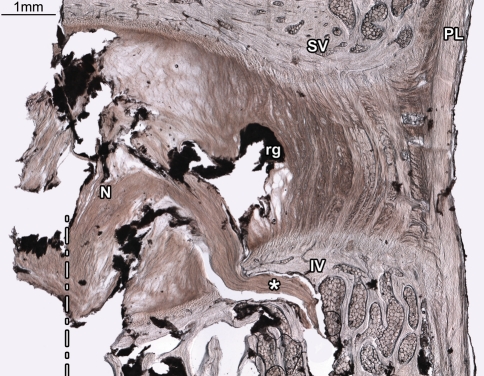
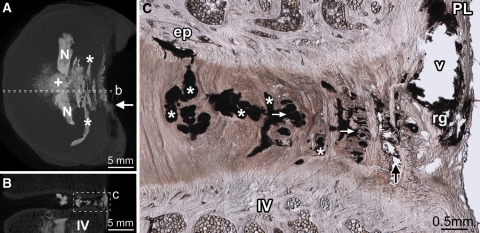
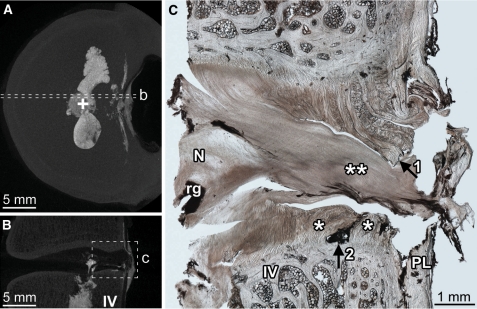
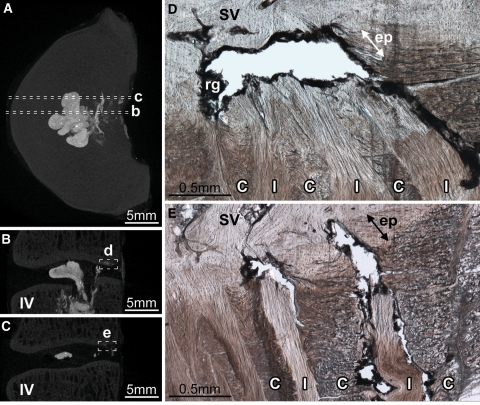
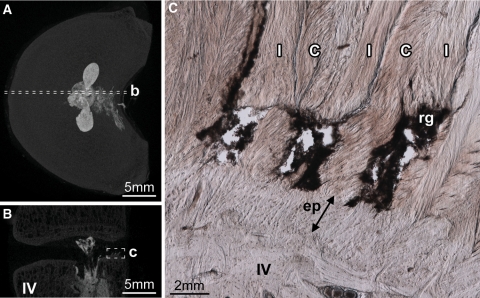
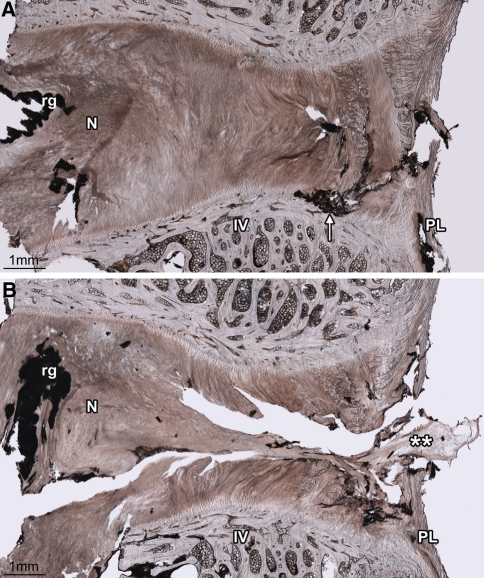
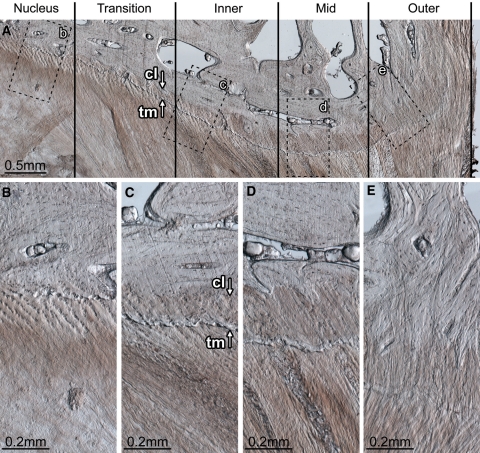
The role of torsion in the mechanical derangement of intervertebral discs remains largely undefined. The current study sought to investigate if torsion, when applied in combination with flexion, affects the internal failure mechanics of the disc wall when exposed to high nuclear pressure. Thirty ovine lumbar motion segments were each positioned in 2 degrees axial rotation plus 7 degrees flexion. Whilst maintained in this posture, the nucleus of each segment was gradually injected with a viscous radio-opaque gel, via an injection screw placed longitudinally within the inferior vertebra, until failure occurred. Segments were then inspected using micro-CT and optical microscopy in tandem. Five motion segments failed to pressurize correctly. Of the remaining 25 successfully tested motion segments, 17 suffered vertebral endplate rupture and 8 suffered disc failure. Disc failure occurred in mature motion segments significantly more often than immature segments. The most common mode of disc failure was a central posterior radial tear involving a systematic annulus-endplate-annulus failure pattern. The endplate portion of these radial tears often propagated contralateral to the direction of applied axial rotation, and, at the lateral margin, only those fibres inclined in the direction of the applied torque were affected. Apart from the 2 degrees of applied axial rotation, the methods employed in this study replicated those used in a previously published study. Consequently, the different outcome obtained in this study can be directly attributed to the applied axial rotation. These inter-study differences show that when combined with flexion, torsion markedly reduces the nuclear pressure required to form clinically relevant radial tears that involve cartilaginous endplate failure. Conversely, torsion appears to increase the disc wall's resistance to radial tears that do not involve cartilaginous endplate failure, effectively halving the disc wall's overall risk of rupture.
Figures
References
-
- Farfan HF. Effects of torsion on the intervertebral joints. Can J Surg. 1969;12:336–341. - PubMed
-
- Farfan HF, Cossette JW, Robertson GH, Wells RV, Kraus H. The effects of torsion on the lumbar intervertebral joints: the role of torsion in the production of disc degeneration. J Bone Joint Surg Am. 1970;52:468–497. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
