

Review
doi: 10.1053/j.ackd.2010.01.005.
Evaluation and management of pain in autosomal dominant polycystic kidney disease
Affiliations
- PMID: 20439087
- PMCID: PMC4144785
- DOI: 10.1053/j.ackd.2010.01.005
Item in Clipboard
Review
Evaluation and management of pain in autosomal dominant polycystic kidney disease
Adv Chronic Kidney Dis.
2010 May.
Abstract
Transient episodes of pain are common in autosomal dominant polycystic kidney disease (ADPKD). A small fraction of patients have disabling chronic pain. In this review, we discuss the etiologies of pain in ADPKD; review how ADPKD patients should be assessed; and discuss medical, surgical, and other management options.
Copyright 2010 National Kidney Foundation, Inc. All rights reserved.
Figures
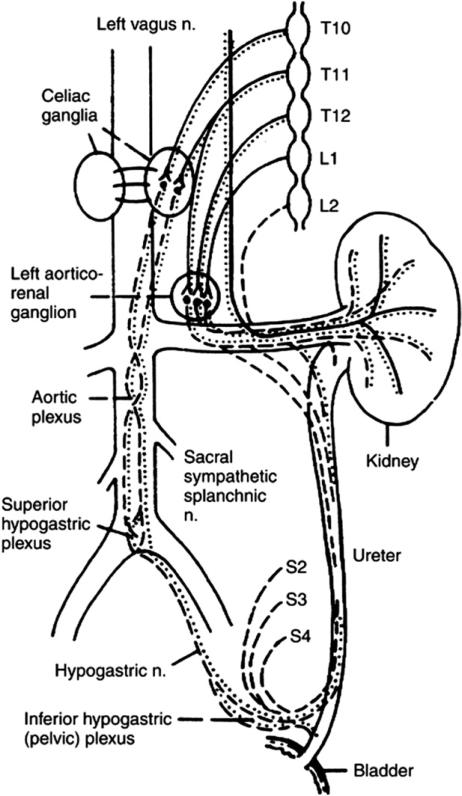
The sympathetic, parasympathetic and sensory innervation of the kidney. Sympathetic fibers from the spinal cord run to the sympathetic chain and, thereafter, via the splanchnic nerves, synapse in the celiac ganglion. The splanchnic nerves lie medial to the sympathetic trunk over the bodies of the thoracic vertebra. Solid line; sympathetic component; dotted line parasympathetic nerve supply; dashed line-afferent sensory fibers and these travel with the autonomic nerves. (By permission of Mayo Foundation for Medical Education and Research, as adapted from Ansell).

A sequential approach to pain management in polycystic kidney disease patients. The first step is to set expectations that pain may not be “cured,” but there will be adaptations that will allow the patient to adjust to the chronic pain. Combining different modalities may be needed for refractory pain. (Reprinted with permission.1).
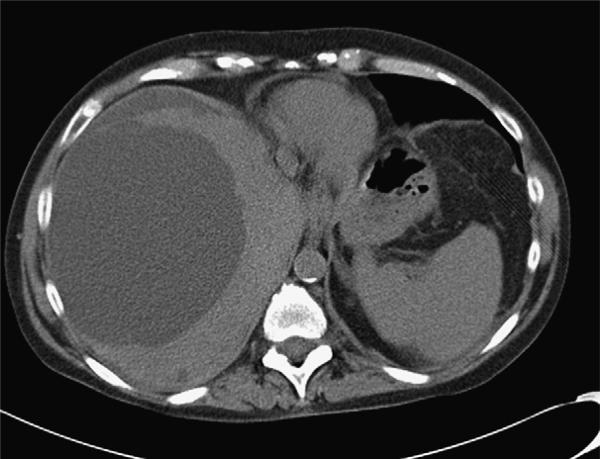
A CT scan of a 59-year-old patient with ADPKD with a dominant right lobe of liver cyst (13 cm in diameter). This patient was managed initially with aspiration of the large cyst shown here. No sclerosis was performed, and the cyst fluid refilled the cyst within 3 months enlarging to 17-cm diameter. She then underwent laparoscopic right-lobe cyst fenestration and remained symptom free for a further 16 months.

The CT scan shows location of larger right upper lobe liver cyst in a 39-year-old female patient with autosomal dominant polycystic liver disease. Images are shown (before and after) 1,100 mL of fluid was aspirated from the cyst without apparent complication under CT guidance; 150 mL of saline and contrast were then reinjected into the cyst (second image). Imaging of the entire liver was then performed that showed no evidence of extravasation from the cyst or connection to the biliary tree. This material was then removed from the cyst, and 20 mL of alcohol were used to sclerose the liver cyst over a 15-minute period. Alcohol was then removed from the cyst. The patient tolerated the procedure well.
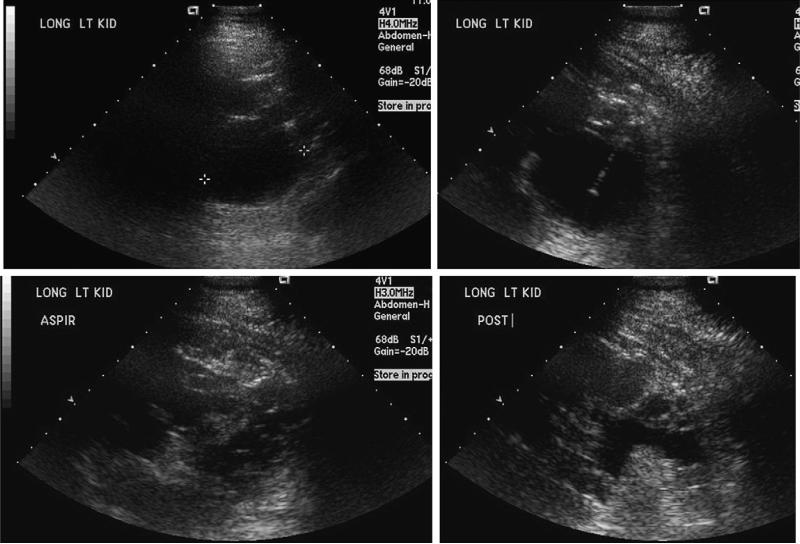
Ultrasound-guided left kidney cyst aspiration and cyst sclerosis for kidney pain in an opiate-dependent 39-year-old man with ADPKD and chronic left kidney pain. He had cyst fenestration surgery 1 year prior where 156 cysts removed from the left kidney. Subsequently, aspiration the largest cyst was drained on the left kidney, and the procedure was a failure in terms of pain. He reported exacerbations of acute pain due to cyst rupture occurring averaging monthly. The dominant 6-cm cyst in the posterior superior aspect of the left kidney seemed to correlate with this patient's left kidney pain (marked with cursors 1 1). Using ultrasound guidance, sterile technique, local anesthetic (1% lidocaine containing bicarbonate), and intravenous sedation, a catheter was advanced into this cyst and ~50 mL of yellow fluid was removed. Next, 20 mL of 95% sterile ethanol was instilled into the cyst under real-time ultra-sound guidance. This was left in place for 8 minutes, at which point a total of 40 mL of fluid was removed, completely decompressing the cyst.
References
-
- Bajwa ZH, Gupta S, Warfield CA, Steinman T. Pain management in polycystic kidney disease. Kidney Int. 2001;60:1631–1644. - PubMed
-
- Bajwa ZH, Sial KA, Malik AB, Steinman TI. Pain patterns in patients with polycystic kidney disease. Kidney Int. 2004;66:1561–1569. - PubMed
-
- Dalgaard OZ. Bilateral polycystic disease of the kidneys: A follow-up of two hundred and eighty-four patients and their families. Acta Med Scand. 1957;328(suppl):1–255. - PubMed
-
- Gabow PA. Autosomal dominant polycystic kidney disease–more than a renal disease. Am J Kidney Dis. 1990;16:403–413. - PubMed
-
- Grantham JJ. Renal pain in polycystic kidney disease: When the hurt won't stop. J Am Soc Nephrol. 1992;2:1161–1162. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
