

Synovial tissue hypoxia and inflammation in vivo
- PMID: 20439288
- PMCID: PMC2946116
- DOI: 10.1136/ard.2009.119776
Synovial tissue hypoxia and inflammation in vivo
Abstract
Introduction: Hypoxia is a microenvironmental feature in the inflamed joint, which promotes survival advantage for cells. The aim of this study was to examine the relationship of partial oxygen pressure in the synovial tissue (tPO(2)) in patients with inflammatory arthritis with macroscopic/microscopic inflammation and local levels of proinflammatory mediators.
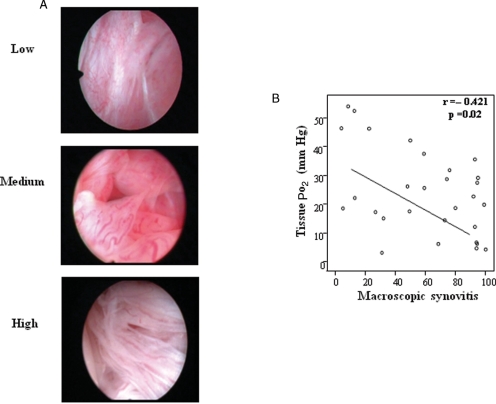
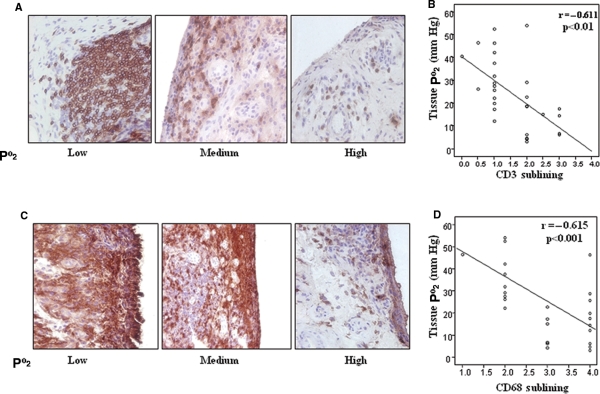
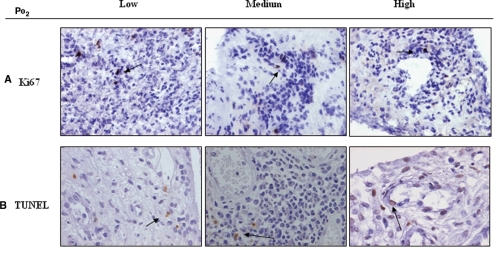
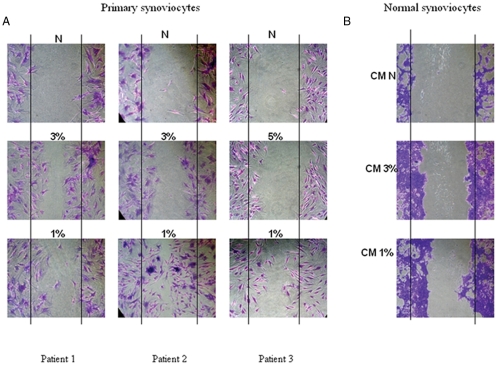
Methods: Patients with inflammatory arthritis underwent full clinical assessment and video arthroscopy to quantify macroscopic synovitis and measure synovial tPO(2) under direct visualisation. Cell specific markers (CD3 (T cells), CD68 (macrophages), Ki67 (cell proliferation) and terminal deoxynucleotidyl transferase dUTP nick end labelling (cell apoptosis)) were quantified by immunohistology. In vitro migration was assessed in primary and normal synoviocytes (synovial fibroblast cells (SFCs)) using a wound repair scratch assay. Levels of tumour necrosis factor alpha (TNFalpha), interleukin 1beta (IL1beta), interferon gamma (IFNgamma), IL6, macrophage inflammatory protein 3alpha (MIP3alpha) and IL8 were quantified, in matched serum and synovial fluid, by multiplex cytokine assay and ELISA.
Results: The tPO(2) was 22.5 (range 3.2-54.1) mm Hg and correlated inversely with macroscopic synovitis (r=-0.421, p=0.02), sublining CD3 cells (-0.611, p<0.01) and sublining CD68 cells (r=-0.615, p<0.001). No relationship with cell proliferation or apoptosis was found. Primary and normal SFCs exposed to 1% and 3% oxygen (reflecting the median tPO(2) in vivo) induced cell migration. This was coupled with significantly higher levels of synovial fluid tumour necrosis factor alpha (TNFalpha), IL1beta, IFNgamma and MIP3alpha in patients with tPO(2) <20 mm Hg (all p values <0.05).
Conclusions: This is the first study to show a direct in vivo correlation between synovial tPO(2), inflammation and cell migration, thus it is proposed that hypoxia is a possible primary driver of inflammatory processes in the arthritic joint.
Conflict of interest statement
Figures

References
-
- Alarcón GS. Epidemiology of rheumatoid arthritis. Rheum Dis Clin North Am 1995;21:589–604 - PubMed
-
- O'Neill T, Silman AJ. Psoriatic arthritis. Historical background and epidemiology. Baillieres Clin Rheumatol 1994;8:245–61 - PubMed
-
- Harris ED Jr Rheumatoid arthritis. Pathophysiology and implications for therapy. N Engl J Med 1990;322:1277–89 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
