

Retrospective analysis of emergency department ultrasound for acute appendicitis
- PMID: 20440399
- PMCID: PMC2860420
Retrospective analysis of emergency department ultrasound for acute appendicitis
Abstract
Objectives: To determine whether emergency physicians (EPs) who have skills in the other applications of ultrasound can apply these in appendicitis diagnosis.
Methods: EPs did not have focused training in bedside ultrasound for appendicitis. We identified patients receiving an ED bedside ultrasound evaluation for appendicitis from our ultrasound log. Criterion reference was radiology ultrasound (RUS), CT scan, or pathology report.
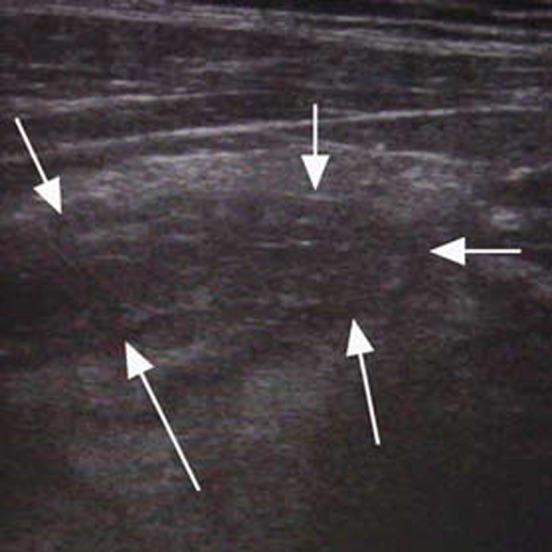
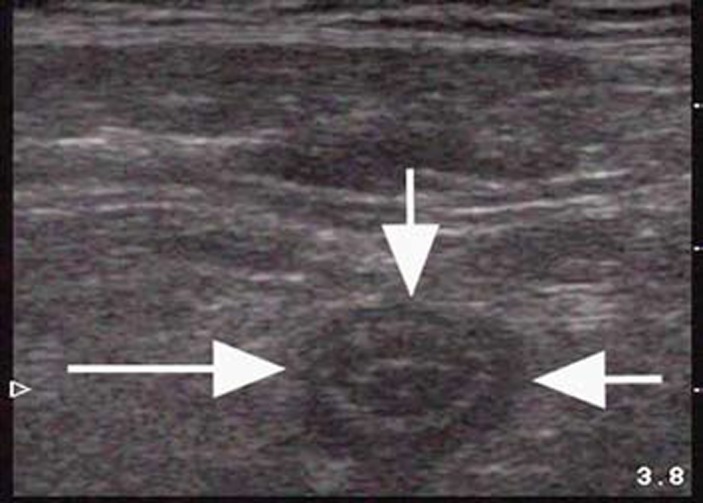
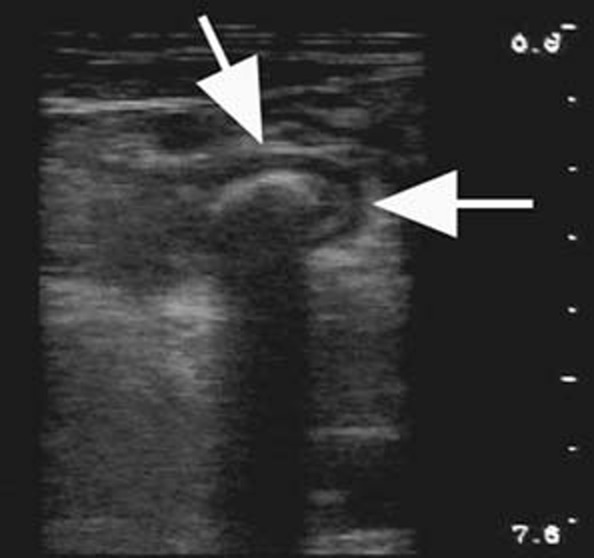
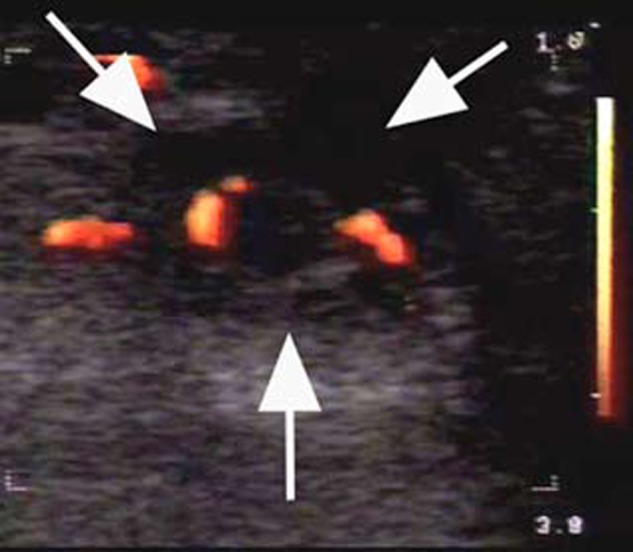
Results: We performed 155 ED ultrasounds for appendicitis. There were 27/155 cases where the ED ultrasound was true positive and agreed with pathology (sensitivity = 39%, 95% CI 28 - 52%). In 42/155 (27%) the ED ultrasound was non-diagnostic (false negative) with pathology positive. In 77 cases the ED ultrasound was true negative with non-visualization of the appendix in concert with non-visualization by RUS or CT scan (specificity = 90%, 95% CI 81-95%). In nine cases (6%), ED ultrasound was falsely positive, compared to CT scan with surgical consult.
Conclusion: ED ultrasound by EPs prior to focused appendicitis ultrasound training is insufficiently accurate.
Keywords: appendicitis; bedside; emergency; retrospective; ultrasound.
Figures
References
-
- Brewer BJ, Golden GT, Hitch DC, Rudolf LE, Wangensteen SL. Abdominal pain. An analysis of 1,000 consecutive cases in a University Hospital emergency room. Am J Surg. 1976;131:219–23. - PubMed
-
- Caterino S, Cavallini M, Meli C, Murante G, Schiffini L, Lotitio S, et al. Acute abdominal pain in emergency surgery. Clinical epidemiologic study of 450 patients. Ann Ital Chir. 1997;68(6):807–17. - PubMed
-
- Simmen HP, Decurtins M, Rotzer A, Duff C, Brutsch HP, Largiader F. Emergency room patients with abdominal pain unrelated to trauma: prospective analysis in a surgical university hospital. Hepatogastroenterology. 1991;38(4):279–82. - PubMed
-
- Paulson EK, Kalady MF, Pappas TN. Clinical practice. Suspected appendicitis. N Engl J Med. 2003 Jan 16;348(3):236–42. - PubMed
-
- Flum DR, McClure TD, Morris A, Koepsell T. Misdiagnosis of appendicitis and the use of diagnostic imaging. J Am Coll Surg. 2005 Dec;201(6):933–9. - PubMed
