

Mechanisms of cerebellar tonsil herniation in patients with Chiari malformations as guide to clinical management
- PMID: 20440631
- PMCID: PMC2887504
- DOI: 10.1007/s00701-010-0636-3
Mechanisms of cerebellar tonsil herniation in patients with Chiari malformations as guide to clinical management
Abstract
Background: The pathogenesis of Chiari malformations is incompletely understood. We tested the hypothesis that different etiologies have different mechanisms of cerebellar tonsil herniation (CTH), as revealed by posterior cranial fossa (PCF) morphology.
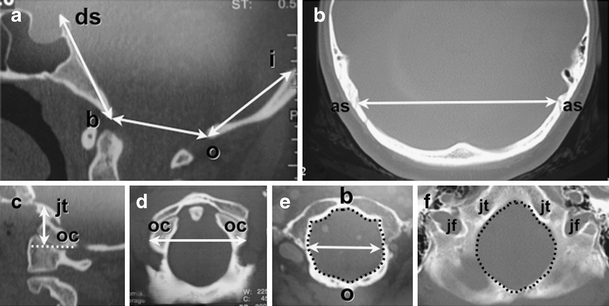
Methods: In 741 patients with Chiari malformation type I (CM-I) and 11 patients with Chiari malformation type II (CM-II), the size of the occipital enchondrium and volume of the PCF (PCFV) were measured on reconstructed 2D-CT and MR images of the skull. Measurements were compared with those in 80 age- and sex-matched healthy control individuals, and the results were correlated with clinical findings.
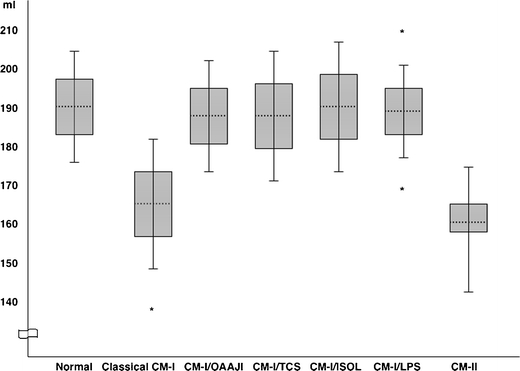
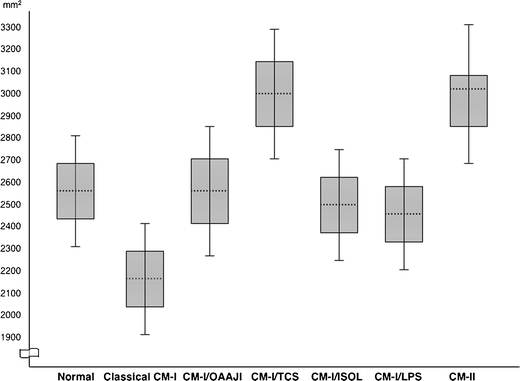
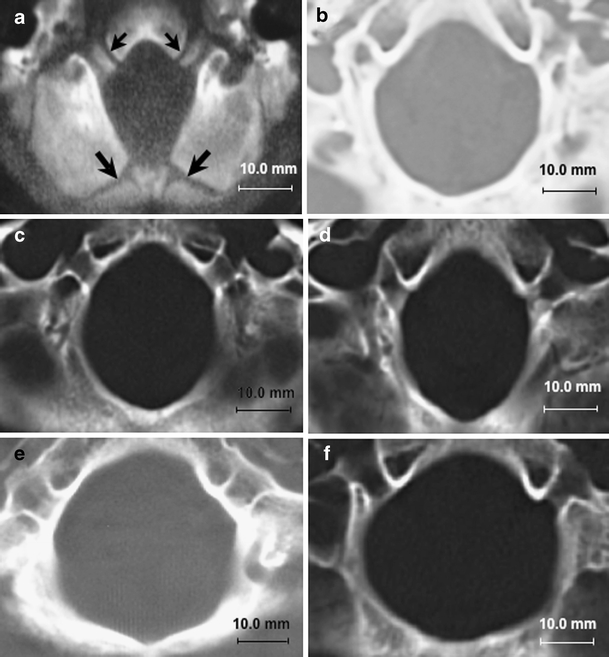
Results: Significant reductions of PCF size and volume were present in 388 patients with classical CM-I, 11 patients with CM-II, and five patients with CM-I and craniosynostosis. Occipital bone size and PCFV were normal in 225 patients with CM-I and occipitoatlantoaxial joint instability, 55 patients with CM-I and tethered cord syndrome (TCS), 30 patients with CM-I and intracranial mass lesions, and 28 patients with CM-I and lumboperitoneal shunts. Ten patients had miscellaneous etiologies. The size and area of the foramen magnum were significantly smaller in patients with classical CM-I and CM-I occurring with craniosynostosis and significantly larger in patients with CM-II and CM-I occurring with TCS.
Conclusions: Important clues concerning the pathogenesis of CTH were provided by morphometric measurements of the PCF. When these assessments were correlated with etiological factors, the following causal mechanisms were suggested: (1) cranial constriction; (2) cranial settling; (3) spinal cord tethering; (4) intracranial hypertension; and (5) intraspinal hypotension.
Conflict of interest statement
None
Figures
References
-
- Abel TJ, Chowdhary A, Gabikian P, Ellenbogen RG, Avellino AM. Acquired Chiari malformation type I associated with a fatty terminal filum. Case report. J Neurosurg. 2006;105:329–332. - PubMed
-
- Chiari H. Über Veränderungen des Kleinhirns in folge von Hydrocephalie des Grosshirns. Dtsch Med Wochenschr. 1891;17:1172–11725. doi: 10.1055/s-0029-1206803. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
