

Lung cancer screening in the randomized Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial
- PMID: 20442215
- PMCID: PMC2873186
- DOI: 10.1093/jnci/djq126
Lung cancer screening in the randomized Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial
Abstract
Background: The 5-year overall survival rate of lung cancer patients is approximately 15%. Most patients are diagnosed with advanced-stage disease and have shorter survival rates than patients with early-stage disease. Although screening for lung cancer has the potential to increase early diagnosis, it has not been shown to reduce lung cancer mortality rates. In 1993, the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial was initiated specifically to determine whether screening would reduce mortality rates from PLCO cancers.
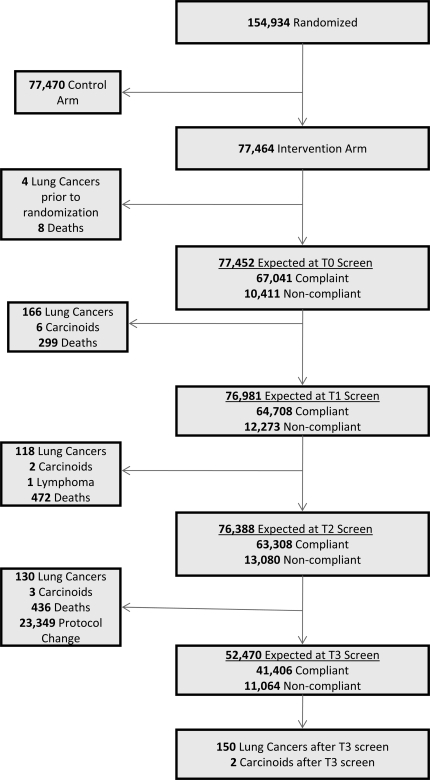
Methods: A total of 77 464 participants, aged 55-74 years, were randomly assigned to the intervention arm of the PLCO Cancer Screening Trial between November 8, 1993, and July 2, 2001. Participants received a baseline chest radiograph (CXR), followed by three annual single-view CXRs at the 10 US screening centers. Cancers were classified as screen detected and nonscreen detected (interval or never screened) and according to tumor histology. The positivity rates of screen-detected cancers and positive predictive values (PPVs) were calculated. Because 51.6% of the participants were current or former smokers, logistic regression analysis was performed to control for smoking status. All statistical tests were two-sided.
Results: Compliance with screening decreased from 86.6% at baseline to 78.9% at the last screening. Overall positivity rates were 8.9% at baseline and 6.6%-7.1% at subsequent screenings; positivity rates increased modestly with smoking risk categories (P(trend) < .001). The PPVs for all participants were 2.0% at baseline and 1.1%, 1.5%, and 2.4% at years 1, 2, and 3, respectively; PPVs in current smokers were 5.9% at baseline and 3.3%, 4.2%, and 5.6% at years 1, 2, and 3, respectively. A total of 564 lung cancers were diagnosed, of which 306 (54%) were screen-detected cancers and 87% were non-small cell lung cancers. Among non-small cell lung cancers, 59.6% of screen-detected cancers and 33.3% of interval cancers were early (I-II) stage.
Conclusions: The PLCO Cancer Screening Trial demonstrated the ability to recruit, retain, and screen a large population over multiple years at multiple centers. A higher proportion of screen-detected lung cancers were early stage, but a conclusion on the effectiveness of CXR screening must await final PLCO results, which are anticipated at the end of 2015.
Figures
Similar articles
-
Baseline chest radiograph for lung cancer detection in the randomized Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial.J Natl Cancer Inst. 2005 Dec 21;97(24):1832-9. doi: 10.1093/jnci/dji430. J Natl Cancer Inst. 2005. PMID: 16368945 Clinical Trial.
-
Association of Nonadherence to Cancer Screening Examinations With Mortality From Unrelated Causes: A Secondary Analysis of the PLCO Cancer Screening Trial.JAMA Intern Med. 2019 Feb 1;179(2):196-203. doi: 10.1001/jamainternmed.2018.5982. JAMA Intern Med. 2019. PMID: 30592477 Free PMC article. Clinical Trial.
-
Interval lung cancers not detected on screening chest X-rays: How are they different?Lung Cancer. 2014 Oct;86(1):41-6. doi: 10.1016/j.lungcan.2014.07.013. Epub 2014 Jul 24. Lung Cancer. 2014. PMID: 25123333 Free PMC article. Clinical Trial.
-
The PLCO Cancer Screening Trial: Background, Goals, Organization, Operations, Results.Rev Recent Clin Trials. 2015;10(3):173-80. doi: 10.2174/1574887110666150730123004. Rev Recent Clin Trials. 2015. PMID: 26238115 Review.
-
The prostate, lung, colorectal, and ovarian cancer screening trial and its associated research resource.J Natl Cancer Inst. 2013 Nov 20;105(22):1684-93. doi: 10.1093/jnci/djt281. Epub 2013 Oct 10. J Natl Cancer Inst. 2013. PMID: 24115361 Free PMC article. Review.
Cited by
-
Potentially functional genetic variants in the complement-related immunity gene-set are associated with non-small cell lung cancer survival.Int J Cancer. 2019 Apr 15;144(8):1867-1876. doi: 10.1002/ijc.31896. Epub 2018 Dec 8. Int J Cancer. 2019. PMID: 30259978 Free PMC article.
-
Novel genetic variants in KIF16B and NEDD4L in the endosome-related genes are associated with nonsmall cell lung cancer survival.Int J Cancer. 2020 Jul 15;147(2):392-403. doi: 10.1002/ijc.32739. Epub 2019 Dec 19. Int J Cancer. 2020. PMID: 31618441 Free PMC article.
-
Novel Variants of ELP2 and PIAS1 in the Interferon Gamma Signaling Pathway Are Associated with Non-Small Cell Lung Cancer Survival.Cancer Epidemiol Biomarkers Prev. 2020 Aug;29(8):1679-1688. doi: 10.1158/1055-9965.EPI-19-1450. Epub 2020 Jun 3. Cancer Epidemiol Biomarkers Prev. 2020. PMID: 32493705 Free PMC article.
-
Potentially functional variants of ERRFI1 in hypoxia-related genes predict survival of non-small cell lung cancer patients.Cancer Med. 2024 Aug;13(15):e70073. doi: 10.1002/cam4.70073. Cancer Med. 2024. PMID: 39096122 Free PMC article.
-
Moving beyond the national lung screening trial: discussing strategies for implementation of lung cancer screening programs.Oncologist. 2013;18(8):941-6. doi: 10.1634/theoncologist.2013-0007. Epub 2013 Jul 19. Oncologist. 2013. PMID: 23873718 Free PMC article.
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55(2):74–108. - PubMed
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58(2):71–96. - PubMed
-
- Goldstraw P, Crowley J, Chansky K, et al. International Association for the Study of Lung Cancer International Staging Committee; Participating Institutions. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol. 2007;2(8):706–714. - PubMed
-
- Naruke T, Goya T, Tsuchiya R, Suemasu K. Prognosis and survival in resected lung carcinoma based on the new international staging system. J Thorac Cardiovasc Surg. 1988;96(3):440–447. - PubMed
-
- Ginsberg RJ, Rubinstein LV. Randomized trial of lobectomy versus limited resection for T1N0 non-small cell lung cancer. Lung Cancer Study Group. Ann Thorac Surg. 1995;60(3):615–623. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
