

Herpes simplex virus pneumonia: high-resolution CT findings
- PMID: 20442279
- PMCID: PMC3473669
- DOI: 10.1259/bjr/51409455
Herpes simplex virus pneumonia: high-resolution CT findings
Abstract
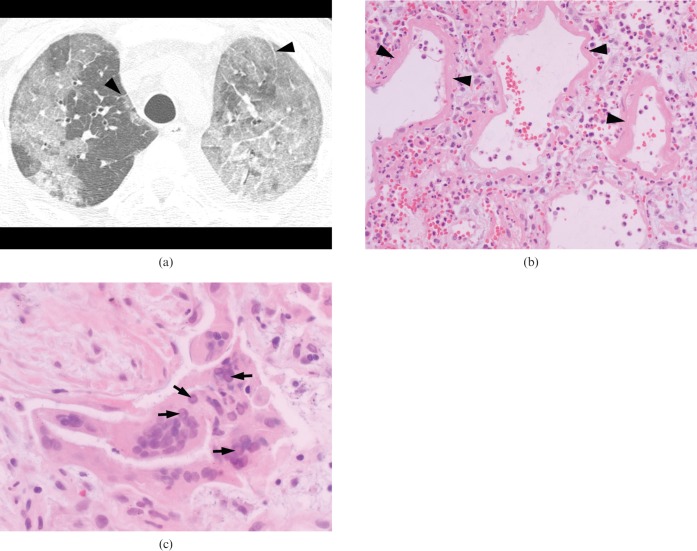
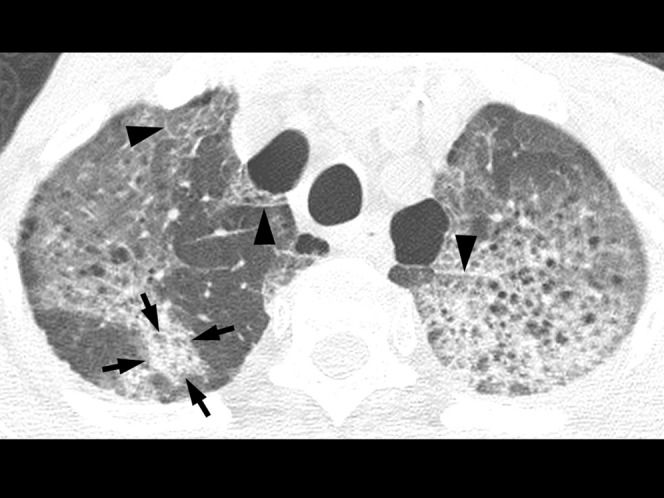
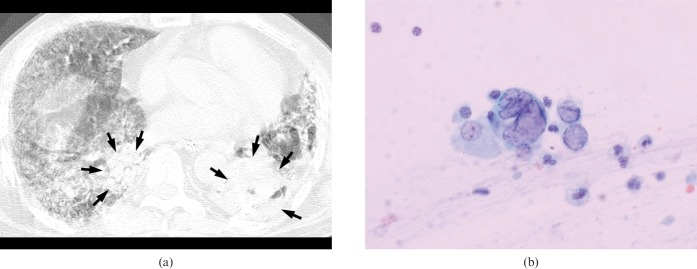
The purpose of this study was to evaluate the high-resolution computed tomographic (HRCT) findings of five adult patients (either immunocompromised or immunocompetent) with herpes simplex virus (HSV) pneumonia. We retrospectively assessed HRCT images of 5 patients (all male patients, age range 39-70 years; mean 62 years) with HSV pneumonia. The specific pathological findings that allowed for a definite diagnosis of HSV pneumonia included the presence of intranuclear inclusion bodies on haematoxylin and eosin staining, or positive immunohistochemical staining. High-resolution CT scans (HiSpeed Advantage or LightSpeed QX/i, GE Healthcare) using 1- or 1.25-mm collimation at 10-mm intervals without intravenous contrast medium injection were assessed, in particular for the presence and distribution of parenchymal abnormalities including ground-glass attenuation, airspace consolidation, nodules and interlobular septal thickening. In two patients, pathological specimens were obtained from open lung biopsy or bronchoscopic biopsy, and were correlated with HRCT findings. Three HRCT patterns of pulmonary abnormalities were identified in our series of HSV pneumonia: predominant areas of diffuse or multifocal ground-glass attenuation, predominant areas of multifocal peribronchial consolidations, and a mixed pattern of both. Histopathologically, areas of ground-glass attenuation seen on HRCT corresponded to diffuse alveolar damage in one patient who underwent open lung biopsy. No specific differences in HRCT findings were seen between the immunocompromised and the immunocompetent patients. In patients suspected of having an acute lower respiratory infection, whether immunocompromised or immunocompetent, a possibility of HSV pneumonia can be included in differential diagnoses when diffuse or multifocal areas of ground-glass attenuation and/or consolidations are seen on HRCT.
Figures

Similar articles
-
Herpes-Simplex-Virus 1 pneumonia in the immunocompromised host: high-resolution CT patterns in correlation to outcome and follow-up.Eur J Radiol. 2012 Apr;81(4):e415-20. doi: 10.1016/j.ejrad.2011.03.014. Epub 2011 Apr 13. Eur J Radiol. 2012. PMID: 21489734
-
Comparison of chest-CT findings of Influenza virus-associated pneumonia in immunocompetent vs. immunocompromised patients.Eur J Radiol. 2015 Jun;84(6):1177-83. doi: 10.1016/j.ejrad.2015.02.014. Epub 2015 Feb 21. Eur J Radiol. 2015. PMID: 25796425
-
Herpes simplex virus 1 pneumonia: patterns on CT scans and conventional chest radiographs.J Comput Assist Tomogr. 1998 Sep-Oct;22(5):795-800. doi: 10.1097/00004728-199809000-00024. J Comput Assist Tomogr. 1998. PMID: 9754119
-
Viral pneumonia after hematopoietic stem cell transplantation: high-resolution CT findings.J Thorac Imaging. 2007 Aug;22(3):292-9. doi: 10.1097/RTI.0b013e31805467f4. J Thorac Imaging. 2007. PMID: 17721347 Review.
-
Imaging of unusual diffuse lung diseases.Curr Opin Pulm Med. 2004 Sep;10(5):383-9. doi: 10.1097/01.mcp.0000134389.50775.b2. Curr Opin Pulm Med. 2004. PMID: 15316437 Review.
Cited by
-
Herpes Simplex Virus (HSV) Pneumonitis as a Late Complication of COVID-19 Infection: A Unique Case Report.Cureus. 2025 Feb 18;17(2):e79228. doi: 10.7759/cureus.79228. eCollection 2025 Feb. Cureus. 2025. PMID: 40115679 Free PMC article.
-
Analysis of 4 imaging features in patients with COVID-19.BMC Med Imaging. 2020 Jul 23;20(1):84. doi: 10.1186/s12880-020-00484-1. BMC Med Imaging. 2020. PMID: 32703209 Free PMC article.
-
Ground-glass opacity (GGO): a review of the differential diagnosis in the era of COVID-19.Jpn J Radiol. 2021 Aug;39(8):721-732. doi: 10.1007/s11604-021-01120-w. Epub 2021 Apr 26. Jpn J Radiol. 2021. PMID: 33900542 Free PMC article. Review.
-
The importance in early identification of a herpetic endobronchial mass.Respir Med Case Rep. 2021 Jul 27;34:101483. doi: 10.1016/j.rmcr.2021.101483. eCollection 2021. Respir Med Case Rep. 2021. PMID: 34466378 Free PMC article.
-
Secondary pneumonia from herpes simplex is not so simple: A case report.SAGE Open Med Case Rep. 2024 May 27;12:2050313X241256858. doi: 10.1177/2050313X241256858. eCollection 2024. SAGE Open Med Case Rep. 2024. PMID: 38812833 Free PMC article.
References
-
- Aquino SL, Dunagan DP, Chiles C, Haponik EF. Herpes simplex virus 1 pneumonia: patterns on CT scans and conventional chest radiographs. J Comput Assist Tomogr 1998;22:795–800 - PubMed
-
- Gasparetto EL, Escuissato DL, Inoue C, Marchiori E, Muller NL. Herpes simplex virus type 2 pneumonia after bone marrow transplantation: high-resolution CT findings in 3 patients. J Thorac Imaging 2005;20:71–3 - PubMed
-
- Travis WD, Colby TV, Koss MN, Rosado-de-Christenson ML, Muller NL, King TE., Jr Non-neoplastic disorders of the lower respiratory tract. Washington DC, USA: American Registry of Pathology, 2002
-
- Ramsey PG, Fife KH, Hackman RC, Meyers JD, Corey L. Herpes simplex virus pneumonia: clinical, virologic, and pathologic features in 20 patients. Ann Intern Med 1982;97:813–20 - PubMed
-
- Oda Y, Okada Y, Katsuda S, Nakanishi I. Immunohistochemical study on the infection of herpes simplex virus, human cytomegalovirus, and Epstein-Barr virus in secondary diffuse interstitial pneumonia. Hum Pathol 1994;25:1057–62 - PubMed
