

Cerebrospinal T-cell responses aid in the diagnosis of tuberculous meningitis in a human immunodeficiency virus- and tuberculosis-endemic population
- PMID: 20442433
- PMCID: PMC2937246
- DOI: 10.1164/rccm.200912-1931OC
Cerebrospinal T-cell responses aid in the diagnosis of tuberculous meningitis in a human immunodeficiency virus- and tuberculosis-endemic population
Abstract
Rationale: Current tools for the rapid diagnosis of tuberculous meningitis (TBM) are suboptimal. We evaluated the clinical utility of a quantitative RD-1 IFN-gamma T-cell enzyme-linked immunospot (ELISPOT) assay (T-SPOT.TB), using cerebrospinal fluid cells for the rapid immunodiagnosis of TBM.
Objectives: To evaluate the diagnostic utility of the RD1 antigen- specific ELISPOT assay for the diagnosis of tuberculous meningitis.
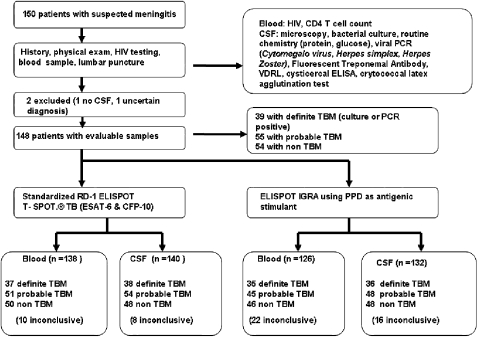
Methods: The ELISPOT assay was evaluated in 150 patients with suspected TBM who were categorized as definite-TBM, probable-TBM, and non-TBM. Culture or polymerase chain reaction positivity for Mycobacerium tuberculosis served as the reference standard. To determine the diagnostic value of the ELISPOT assay, a clinical prediction rule was derived from baseline clinical and laboratory parameters using a multivariable regression model.
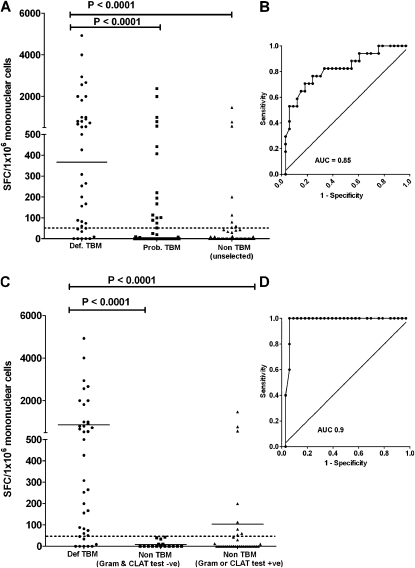
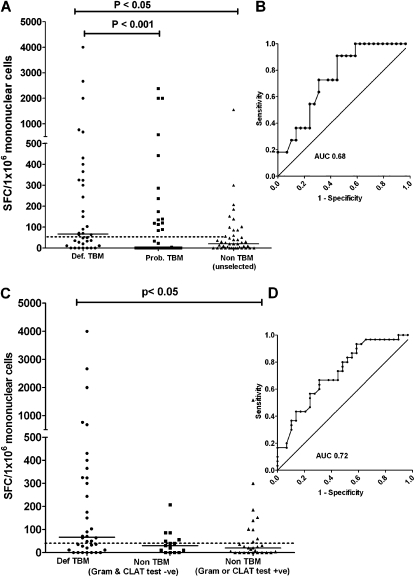
Measurements and main results: A total of 140 patients (81% HIV-infected; median CD4 count, 160 cells/mm(3)) were included in the final analysis. When comparing the definite-TBM (n = 38) and non-TBM groups (n = 48), the ELISPOT assay (cut point of > or =228 spot-forming cells per 1 million mononuclear cells) was a useful rule-in test: sensitivity 58% (95% confidence interval [CI], 41-74); specificity 94% (95% CI, 83-99). However, ELISPOT outcomes improved when other rapid tests were concurrently used to exclude bacterial (Gram stain) and cryptococcal meningitis (latex-agglutination test) within the non-TBM group. Using this approach, the ELISPOT assay (cut point of > or =46 spot-forming cells) was an excellent rule-in test: sensitivity 82% (95% CI, 66-92); specificity 100% (95% CI, 78-100); positive predictive value, 100% (95% CI, 89-100); negative predictive value, 68% (95% CI, 45-86); area under the curve, 0.90. The ELISPOT assay had incremental diagnostic value compared with the clinical prediction rule.
Conclusions: The RD-1 ELISPOT assay, using cerebrospinal fluid mononuclear cells and in conjunction with other rapid confirmatory tests (Gram stain and cryptococcal latex-agglutination test), is an accurate rapid rule-in test for TBM in a TB and HIV endemic setting.
Figures
Similar articles
-
Comparison of a clinical prediction rule and a LAM antigen-detection assay for the rapid diagnosis of TBM in a high HIV prevalence setting.PLoS One. 2010 Dec 22;5(12):e15664. doi: 10.1371/journal.pone.0015664. PLoS One. 2010. PMID: 21203513 Free PMC article.
-
Diagnostic usefulness of T-cell based assays for tuberculous meningitis in HIV-uninfected patients.J Infect. 2016 Apr;72(4):486-97. doi: 10.1016/j.jinf.2016.01.012. Epub 2016 Feb 3. J Infect. 2016. PMID: 26851800
-
Rapid diagnosis of tuberculous meningitis by T cell-based assays on peripheral blood and cerebrospinal fluid mononuclear cells.Clin Infect Dis. 2010 May 15;50(10):1349-58. doi: 10.1086/652142. Clin Infect Dis. 2010. PMID: 20380567
-
[Evolution of IGRA researches].Kekkaku. 2008 Sep;83(9):641-52. Kekkaku. 2008. PMID: 18979999 Review. Japanese.
-
Diagnostic accuracy of Xpert MTB/RIF for tuberculous meningitis: systematic review and meta-analysis.Trop Med Int Health. 2021 Feb;26(2):122-132. doi: 10.1111/tmi.13525. Epub 2020 Nov 30. Trop Med Int Health. 2021. PMID: 33164243 Free PMC article.
Cited by
-
Diagnostic accuracy of quantitative PCR (Xpert MTB/RIF) for tuberculous meningitis in a high burden setting: a prospective study.PLoS Med. 2013 Oct;10(10):e1001536. doi: 10.1371/journal.pmed.1001536. Epub 2013 Oct 22. PLoS Med. 2013. PMID: 24167451 Free PMC article.
-
A New Scoring System to Differentially Diagnose and Distinguish Tuberculous Meningitis and Bacterial Meningitis in South China.Front Neurol. 2022 Mar 30;13:830969. doi: 10.3389/fneur.2022.830969. eCollection 2022. Front Neurol. 2022. PMID: 35432172 Free PMC article.
-
The immunology of tuberculosis: from bench to bedside.Respirology. 2010 Apr;15(3):433-50. doi: 10.1111/j.1440-1843.2010.01739.x. Respirology. 2010. PMID: 20415982 Free PMC article. Review.
-
Comparison of a clinical prediction rule and a LAM antigen-detection assay for the rapid diagnosis of TBM in a high HIV prevalence setting.PLoS One. 2010 Dec 22;5(12):e15664. doi: 10.1371/journal.pone.0015664. PLoS One. 2010. PMID: 21203513 Free PMC article.
-
Tuberculosis Meningitis.Curr Infect Dis Rep. 2017 Sep 11;19(11):39. doi: 10.1007/s11908-017-0595-4. Curr Infect Dis Rep. 2017. PMID: 28895024 Review.
References
-
- WHO. Global tuberculosis control: surveillance, planning, financing. WHO report, 2009 [accessed October 20, 2009]. Available from: http://www.WHO/HTM/TB/2008.393
-
- CDC. Extrapulmonary tuberculosis cases and percentages by site of disease: reporting areas. Centers for disease control and prevention, Atlanta, GA [accessed October 30, 2000]. Available from: www.cdc.gov/tb/surv/surv2005/PDF/table27.pdf
-
- Phypers M, Harris T, Power C. CNS tuberculosis: a longitudinal analysis of epidemiological and clinical features. Int J Tuberc Lung Dis 2006;10:99–103. - PubMed
-
- Peto HM, Pratt RH, Harrington TA, LoBue PA, Armstrong LR. Epidemiology of extrapulmonary tuberculosis in the United States, 1993–2006. Clin Infect Dis 2009;49:1350–1357. - PubMed
-
- Braunwald E, Fauchi AS, Kasper DL, Hauser SL, Longo DL, Jameson JL. Harrisons's principles of internal medicine. New York: McGraw-Hill; 2001.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
