

Determinants of survival in very low birth weight neonates in a public sector hospital in Johannesburg
- PMID: 20444296
- PMCID: PMC2885379
- DOI: 10.1186/1471-2431-10-30
Determinants of survival in very low birth weight neonates in a public sector hospital in Johannesburg
Abstract
Background: Audit of disease and mortality patterns provides essential information for health budgeting and planning, as well as a benchmark for comparison. Neonatal mortality accounts for about 1/3 of deaths < 5 years of age and very low birth weight (VLBW) mortality for approximately 1/3 of neonatal mortality. Intervention programs must be based on reliable statistics applicable to the local setting; First World data cannot be used in a Third World setting. Many neonatal units participate in the Vermont Oxford Network (VON); limited resources prevent a significant number of large neonatal units from developing countries taking part, hence data from such units is lacking. The purpose of this study was to provide reliable, recent statistics relevant to a developing African country, useful for guiding neonatal interventions in that setting.
Methods: This was a retrospective chart review of 474 VLBW infants admitted within 24 hours of birth, between 1 July 2006 and 30 June 2007, to the neonatal unit of Charlotte Maxeke Johannesburg Academic Hospital (CMJAH) in Johannesburg, South Africa. Binary outcome logistic regression on individual variables and multiple logistic regression was done to identify those factors determining survival.
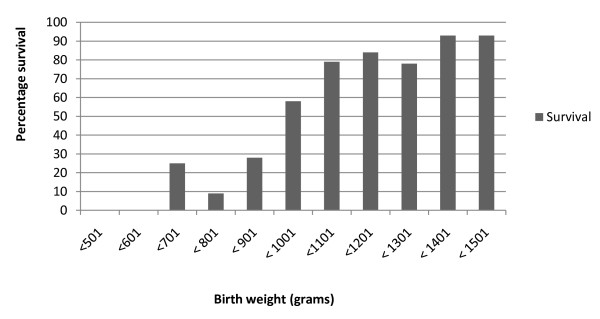
Results: Overall survival was 70.5%. Survival of infants below 1001 grams birth weight was 34.9% compared to 85.8% for those between 1001 and 1500 grams at birth. The main determinant of survival was birth weight with an adjusted survival odds ratio of 23.44 (95% CI: 11.22 - 49.00) for babies weighing between 1001 and 1500 grams compared to those weighing below 1001 grams. Other predictors of survival were gender (OR 3. 21; 95% CI 1.6 - 6.3), birth before arrival at the hospital (BBA) (OR 0.23; 95% CI: 0.08 - 0.69), necrotising enterocolitis (NEC) (OR 0.06; 95% CI: 0.02 - 0.20), hypotension (OR 0.05; 95% CI 0.01 - 0.21) and nasal continuous positive airways pressure (NCPAP) (OR 4.58; 95% CI 1.58 - 13.31).
Conclusions: Survival rates compare favourably with other developing countries, but can be improved; especially in infants < 1001 grams birth weight. Resources need to be allocated to preventing the birth of VLBW babies outside hospital, early neonatal resuscitation, provision of NCPAP and prevention of NEC.
References
-
- United Nations. Reduce Child Mortality. The Millennium Development Goals Report New York. 2008. pp. 21–3.
-
- Patrick ME. In: Saving Children 2006: A survey of child healthcare in South Africa. Stephen CRPM, editor. Pretoria: University of Pretoria, MRC, CDC; 2008. Neonatal deaths: Do they count? pp. 81–5.
-
- Litt R, Seidman DS, Gross-Tsur V, Dollberg S, Gale R. A 2-year prospective study of very low birth weight infants. Isr J Med Sci. 1992;28:783–8. - PubMed
-
- de Vonderweid U, Carta A, Chiandotto V, Chiappe F, Chiappe S, Colarizi P. Italian Multicenter Study on Very Low Birth Weight Babies. Ann IST Super Sanita. 1991;27:633–50. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
