

Fibroblast growth factor-23 in early chronic kidney disease: additional support in favor of a phosphate-centric paradigm for the pathogenesis of secondary hyperparathyroidism
- PMID: 20448073
- PMCID: PMC2893066
- DOI: 10.2215/CJN.08241109
Fibroblast growth factor-23 in early chronic kidney disease: additional support in favor of a phosphate-centric paradigm for the pathogenesis of secondary hyperparathyroidism
Abstract
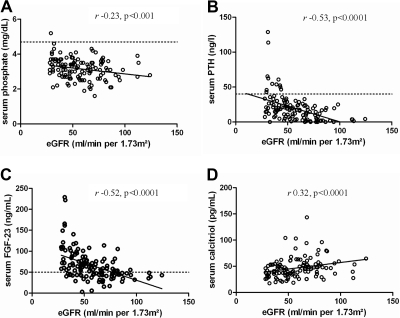
Background and objectives: The discovery of fibroblast growth factor-23 (FGF-23) and the elucidation of its function as a phosphaturic and 1,25(OH)2VitD counter-regulatory hormone provides a new conceptual framework for the understanding of the pathogenesis of secondary hyperparathyroidism. This study aims to elucidate the complex associations between FGF-23, parathyroid hormone (PTH), 1,25(OH)2D, and phosphate in patients with early-stage chronic kidney disease (CKD) and to provide clinical evidence in favor of the new phosphate-centric paradigm for the pathogenesis of secondary hyperparathyroidism.
Design, setting, participants, & measurements: Serum biointact PTH and FGF-23, 25(OH)D, 1,25(OH)2D, calcium, phosphate, 24-hour urine excretion of phosphate and calcium, and urinary fractional excretion of phosphate were determined in a cross-sectional study including 125 patients with CKD stages 1 to 3.
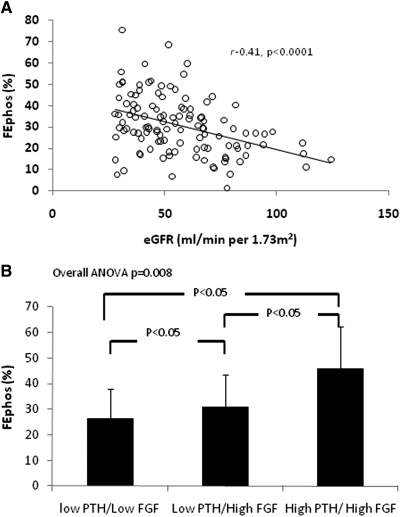
Results: Serum phosphate levels showed an inverse association with estimated GFR (eGFR), but were within the normal range in all but one patient. FGF-23 and PTH were inversely associated with eGFR, even in the subgroup of patients with CKD stages 1 and 2. High FGF-23 levels were significantly more prevalent than high PTH levels. The urinary fractional excretion of phosphate was highest in patients with both a high serum FGF-23 and PTH level. Increased FGF-23 and phosphate and decreased 25(OH)D were independently associated with decreased 1,25(OH)2D.
Conclusions: Our data are in favor of the new paradigm for the pathogenesis of secondary hyperparathyroidism according to which a reduced phosphate excretion capacity is the principal abnormality that initiates secondary hyperparathyroidism.
Trial registration: ClinicalTrials.gov NCT00441623.
Figures
References
-
- Nemere I: The ins and outs of phosphate homeostasis. Kidney Int 72: 140–142, 2007 - PubMed
-
- Craver L, Marco MP, Martinez I, Rue M, Borras M, Martin ML, Sarro F, Valdivielso JM, Fernandez E: Mineral metabolism parameters throughout chronic kidney disease stages 1–5—achievement of K/DOQI target ranges. Nephrol Dial Transplant 22: 1171–1176, 2007 - PubMed
-
- Gutierrez O, Isakova T, Rhee E, Shah A, Holmes J, Collerone G, Juppner H, Wolf M: Fibroblast growth factor-23 mitigates hyperphosphatemia but accentuates calcitriol deficiency in chronic kidney disease. J Am Soc Nephrol 16: 2205–2215, 2005 - PubMed
-
- Levin A, Bakris GL, Molitch M, Smulders M, Tian J, Williams LA, Andress DL: Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: Results of the study to evaluate early kidney disease. Kidney Int 71: 31–38, 2007 - PubMed
-
- Berndt T, Kumar R: Phosphatonins and the regulation of phosphate homeostasis. Annu Rev Physiol 69: 341–359, 2007 - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
