

From laboratory science to six emergency medical services systems: New understanding of the physiology of cardiopulmonary resuscitation increases survival rates after cardiac arrest
- PMID: 20449900
- PMCID: PMC3429344
- DOI: 10.1097/ccm.0b013e31818a7e56
From laboratory science to six emergency medical services systems: New understanding of the physiology of cardiopulmonary resuscitation increases survival rates after cardiac arrest
Abstract
Objective: The purpose of this study is to: 1) describe a newly mechanism of blood flow to the brain during cardiopulmonary resuscitation using the impedance threshold device in a piglet model of cardiac arrest, and 2) describe the survival benefits in humans of applying all of the highly recommended changes in the 2005 guidelines related to increasing circulation during cardiopulmonary resuscitation, including use of the impedance threshold device, from six emergency medical services systems in the United States.
Design: Animal studies prospective trial with each piglet serving as its own control. Historical controls were used for the human studies.
Subjects: Piglets and patients with out-of-hospital cardiac arrest.
Interventions: Piglets (10-12 kg) were treated with an active (n = 9) or sham (n = 9) impedance threshold device after 6 mins of ventricular fibrillation. Humans were treated with cardiopulmonary resuscitation per the American Heart Association 2005 guidelines and the impedance threshold device.
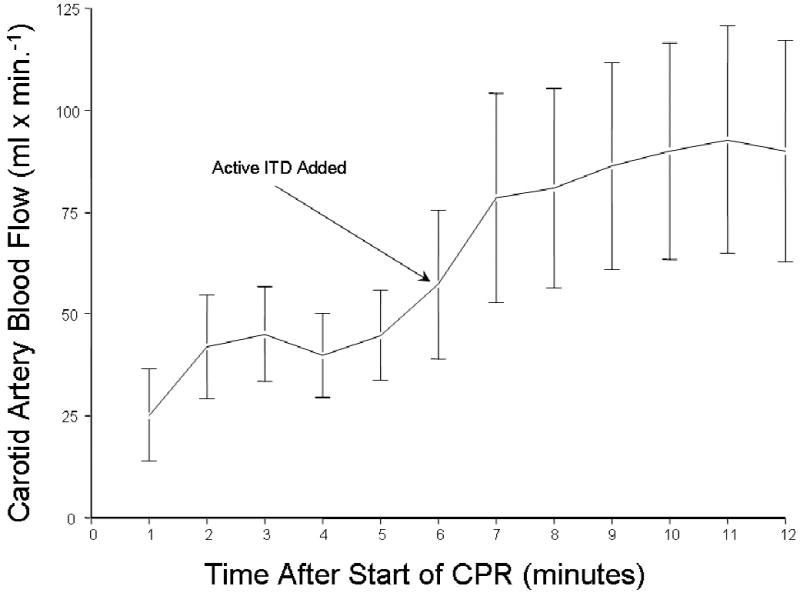
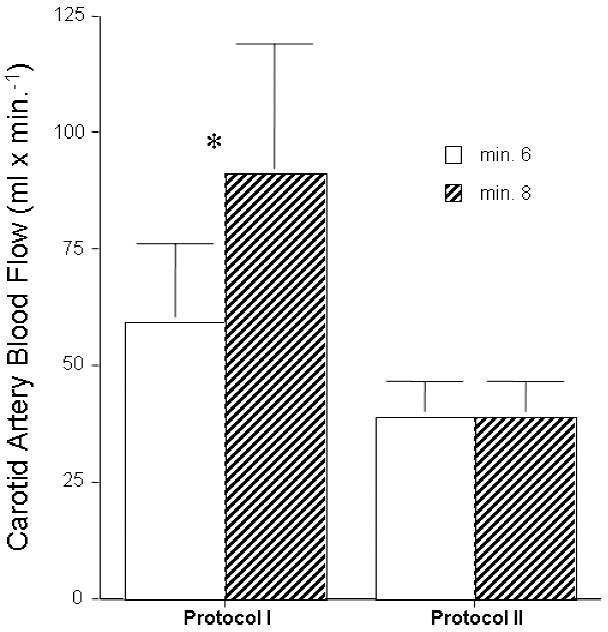
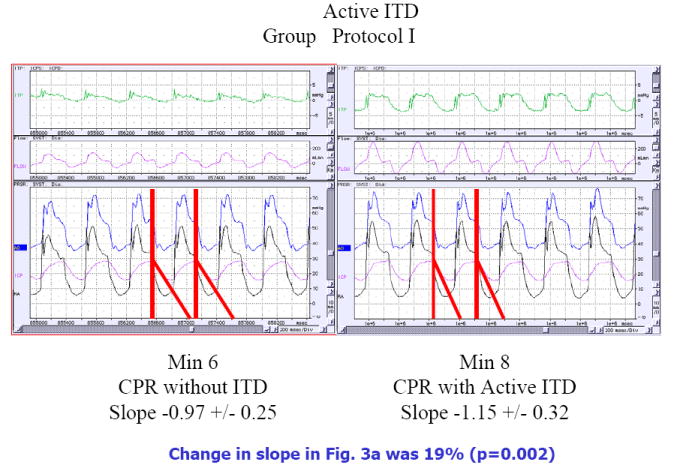
Animals: The primary endpoint in the piglet study was carotid blood flow which increased from 59 mL/min without an impedance threshold device to 91 mL/min (p = 0.017) with impedance threshold device use. Airway pressures during the chest recoil phase decreased from -0.46 mm Hg to -2.59 mm Hg (p = 0.0006) with the active impedance threshold device. Intracranial pressure decreased more rapidly and to a greater degree during the decompression phase of cardiopulmonary resuscitation with the active impedance threshold device. Humans: Conglomerate quality assurance data were analyzed from six emergency medical services systems in the United States serving a population of approximately 3 million people. There were 920 patients treated for cardiac arrest after implementation of the 2005 American Heart Association guidelines, including impedance threshold device use, and 1750 patients in the control group during the year before implementation. Demographics were similar between the two groups. Survival to hospital discharge was 9.3% in the control group versus 13.6% in the intervention group. The odds ratio, 95% confidence interval, and p value were 1.54 (1.19-1.99) and p = 0.0008, respectively. This survival advantage was conferred to patients with a presenting cardiac arrest rhythm of ventricular fibrillation (28.5% vs. 18.0%, p = 0.0008).
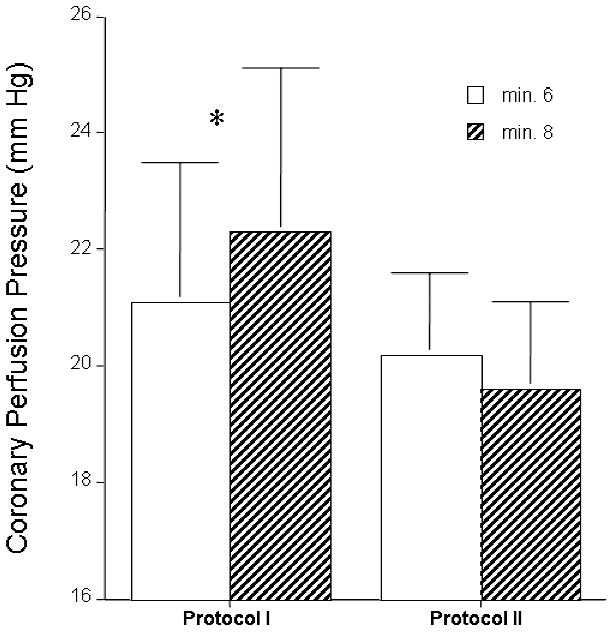
Conclusions: Use of the impedance threshold device in piglets increased carotid blood flow and coronary and cerebral perfusion pressures and reduced intracranial pressure during the decompression phase of cardiopulmonary resuscitation at a faster rate than controls, resulting in a longer duration of time when intracranial pressures are at their nadir. Patients in six emergency medical services systems treated with the impedance threshold device together with the renewed emphasis on more compressions, fewer ventilations, and complete chest wall recoil had a nearly 50% increase in survival rates after out-of-hospital cardiac arrest compared with historical controls.
Figures


References
-
- Kouwenhoven WB, Jude JR, Knickerbocker GG. Closed chest cardiac massage. JAMA. 1960;173:1064–1067. - PubMed
-
- Duggal C, Weil MH, Gazmuri RJ, Tang W, Sun S, O’Connell F, Ali M. Regional blood flow during closed-chest cardiac resuscitation in rats. J Appl Physiol. 1993 Jan;74(1):147–52. - PubMed
-
- Andreka P, Frenneaux MP. Haemodynamics of cardiac arrest and resuscitation. Curr Opin Crit Care. 2006 Jun;12(3):198–203. - PubMed
-
- Niemann JT. Cardiopulmonary resuscitation. N Engl J Med. 1992;327:1075–1090. - PubMed
-
- Eisenberg MS, Horwood BT, Cummins RO, et al. Cardiac arrest and resuscitation: a tale of 29 cities. Ann Emerg Med. 1990;19:179–186. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
