

Review
doi: 10.1016/j.mcna.2010.02.009.
Sleep in congestive heart failure
Affiliations
- PMID: 20451026
- PMCID: PMC3424608
- DOI: 10.1016/j.mcna.2010.02.009
Item in Clipboard
Review
Sleep in congestive heart failure
Med Clin North Am.
2010 May.
Abstract
Breathing disorders during sleep are common in congestive heart failure (CHF). Sleep-disordered breathing (SDB) in CHF can be broadly classified as 2 types: central sleep apnea with Cheyne-Stokes breathing, and obstructive sleep apnea. Prevalence of SDB ranges from 47% to 76% in systolic CHF. Treatment of SDB in CHF may include optimization of CHF treatment, positive airway pressure therapy, and other measures such as theophylline, acetazolamide, and cardiac resynchronization therapy. Periodic limb movements are also common in CHF.
Figures
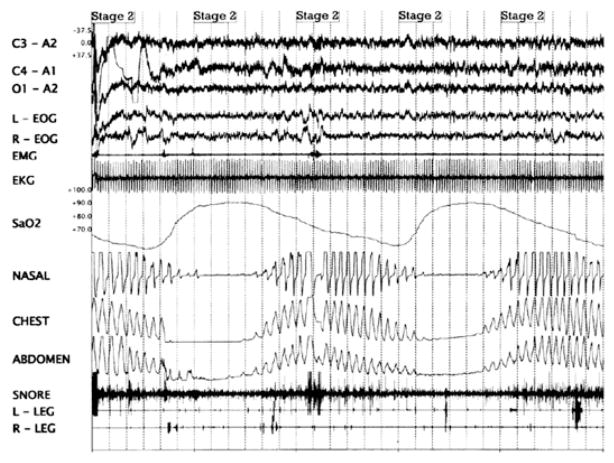
Polysomnogram showing Cheyne-Stokes breathing. There are crescendo-decrescendo changes in tidal volume that result in central apneas (as shown in the chest and abdominal respiratory movements in the polysomnogram).
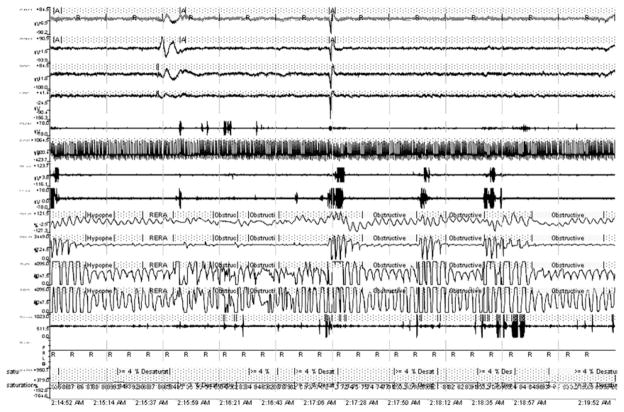
Polysomnogram showing obstructive sleep apnea. There are repetitive episodes of oxygen desaturation episodes despite ongoing respiratory effort (as shown by thoracic and abdominal respiratory movements), and arousals. Apnea exists when airflow is less than 20% of baseline for at least 10 seconds in adults. Hypopnea exists when airflow decreases at least 30% from baseline, there is diminished airflow lasting at least 10 seconds, at least 90% of the duration of diminished airflow is spent with airflow that is at least 30% less than baseline, and decreased airflow is accompanied by at least 4%oxyhemoglobin desaturation. Respiratory effort related arousals (RERAs) exist when there is a sequence of breaths that lasts at least 10 seconds, is characterized by increasing respiratory effort or flattening of the nasal pressure waveform, and leads to an arousal from sleep, but does not meet the criteria of an apnea or hypopnea.
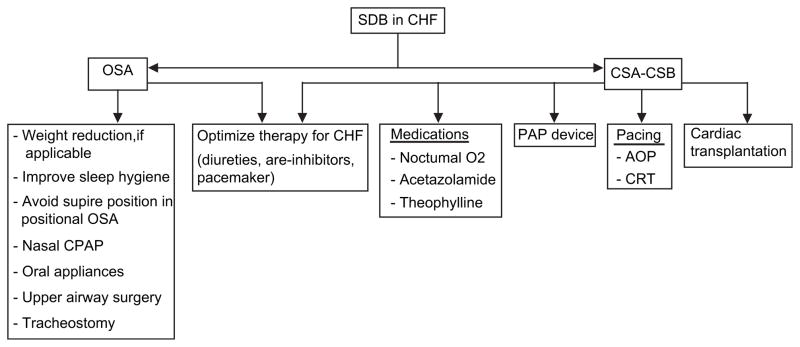
A suggested algorithm for management of sleep-disordered breathing in congestive heart failure.
References
-
- Hunt SA, Baker DW, Chin MH, et al. ACC/AHA Guidelines for the evaluation and management of chronic heart failure in the adult: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2001;104(24):2996–3007. - PubMed
-
- Levy D, Kenechaiah S, Larson MG, et al. Long-term trends in the incidence of and survival with heart failure. N Engl J Med. 2002;347(18):1397–402. - PubMed
-
- Javaheri S, Parker TJ, Liming JD, et al. Sleep apnea in 81 ambulatory male patients with stable heart failure. Types and their prevalences, consequences, and presentations. Circulation. 1998;97(21):2154–9. - PubMed
-
- Tremel F, Pépin JL, Veale D, et al. High prevalence and persistence of sleep apnoea in patients referred for acute left ventricular failure and medically treated over 2 months. Eur Heart J. 1999;20(16):1201–9. - PubMed
-
- Sin DD, Fitzgerald F, Parker JD, et al. Risk factors for central and obstructive sleep apnea in 450 men and women with congestive heart failure. Am J Respir Crit Care Med. 1999;160(4):1101–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
