

Childhood obesity
- PMID: 20451244
- PMCID: PMC3073855
- DOI: 10.1016/S0140-6736(10)60171-7
Childhood obesity
Abstract
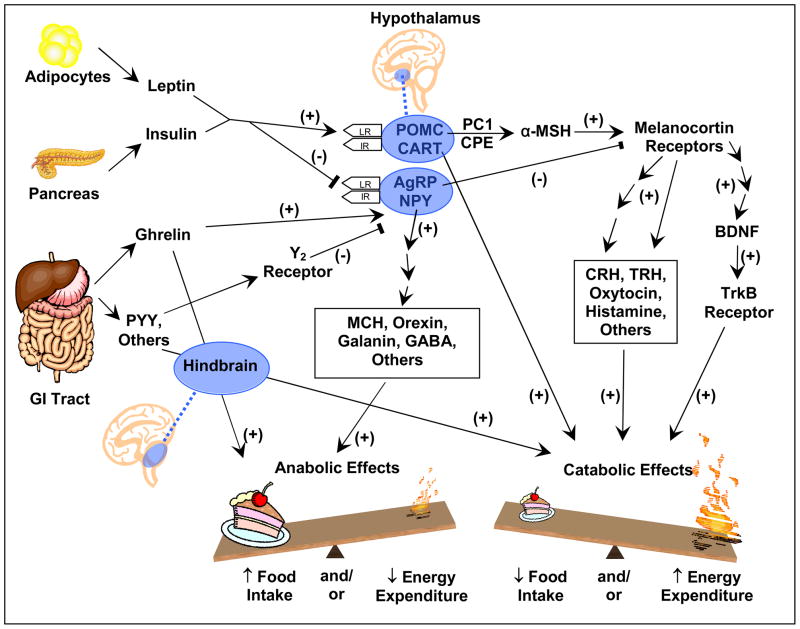
Worldwide prevalence of childhood obesity has increased greatly during the past three decades. The increasing occurrence in children of disorders such as type 2 diabetes is believed to be a consequence of this obesity epidemic. Much progress has been made in understanding of the genetics and physiology of appetite control and from these advances, elucidation of the causes of some rare obesity syndromes. However, these rare disorders have so far taught us few lessons about prevention or reversal of obesity in most children. Calorie intake and activity recommendations need reassessment and improved quantification at a population level because of sedentary lifestyles of children nowadays. For individual treatment, currently recommended calorie prescriptions might be too conservative in view of evolving insight into the so-called energy gap. Although quality of research into both prevention and treatment has improved, high-quality multicentre trials with long-term follow-up are needed. Meanwhile, prevention and treatment approaches to increase energy expenditure and decrease intake should continue. Recent data suggest that the spiralling increase in childhood obesity prevalence might be abating; increased efforts should be made on all fronts to continue this potentially exciting trend.
Copyright 2010 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of interest statement
Dr. Kimm serves as a member of the Medical Advisory Board of the Aspartame Resource Center, from which she received no support for her research or her effort in this manuscript.
Figures
References
-
- Ebbeling CB, Pawlak DB, Ludwig DS. Childhood obesity: public-health crisis, common sense cure. Lancet. 2002;360(9331):473–82. - PubMed
-
- Wang Y, Lobstein T. Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes. 2006;1(1):11–25. - PubMed
-
- Ogden CL, Carroll MD, Flegal KM. High body mass index for age among US children and adolescents, 2003–2006. Jama. 2008;299(20):2401–5. - PubMed
-
- Kipping RR, Jago R, Lawlor DA. Obesity in children. Part 1: Epidemiology, measurement, risk factors, and screening. Bmj. 2008;337:a1824. - PubMed
-
- Sundblom E, Petzold M, Rasmussen F, Callmer E, Lissner L. Childhood overweight and obesity prevalences levelling off in Stockholm but socioeconomic differences persist. Int J Obes (Lond) 2008;32(10):1525–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
