

The neurohormonal regulation of energy intake in relation to bariatric surgery for obesity
- PMID: 20452367
- PMCID: PMC3128515
- DOI: 10.1016/j.physbeh.2010.04.032
The neurohormonal regulation of energy intake in relation to bariatric surgery for obesity
Abstract
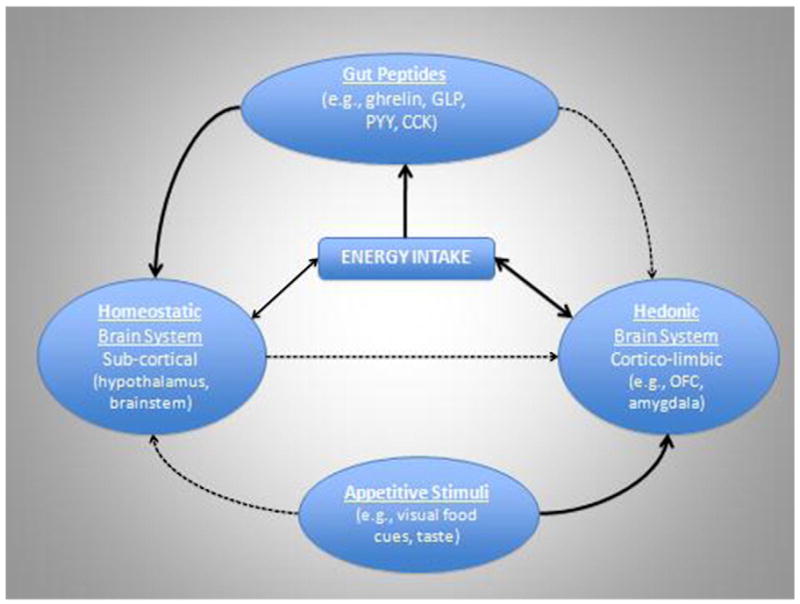
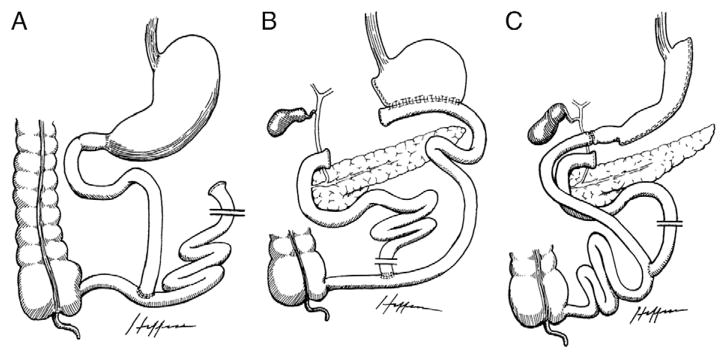
Obesity has reached pandemic proportions, with bariatric surgery representing the only currently available treatment demonstrating long-term effectiveness. Over 200,000 bariatric procedures are performed each year in the US alone. Given the reliable and singular success of bariatric procedures, increased attention is being paid to identifying the accompanying neurohormonal changes that may contribute to the resulting decrease in energy intake. Numerous investigations of postsurgical changes in gut peptides have been conducted, suggesting greater alterations in endocrine function in combination restrictive and malabsorptive procedures (e.g., Roux-en-Y gastric bypass) as compared to purely restrictive procedures (e.g., gastric banding), which may contribute to the increased effectiveness of combination procedures. However, very few studies have been performed and relatively little is known about changes in neural activation that may result from bariatric procedures, which likely interact with changes in gut peptides to influence postsurgical caloric intake. This review provides a background in the neurohormonal regulation of energy intake and discusses how differing forms of bariatric surgery may affect the neurohormonal network, with emphasis on Roux-en-Y gastric bypass, the most commonly performed procedure worldwide. The paper represents an invited review by a symposium, award winner or keynote speaker at the Society for the Study of Ingestive Behavior [SSIB] Annual Meeting in Portland, July 2009.
2010 Elsevier Inc. All rights reserved.
Figures


References
-
- Samuel I, Mason EE, Renquist KE, Huang YH, Zimmerman MB, Jamal M. Bariatric surgery trends: an 18-year report from the International Bariatric Surgery Registry. Am J Surg. 2006;192:657–62. - PubMed
-
- Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults—the evidence report. National Institutes of Health. Obes Res. 1998;6(Suppl 2):51S–209S. - PubMed
-
- Buchwald H, Williams SE. Bariatric surgery worldwide 2003. Obes Surg. 2004;14:1157–64. - PubMed
-
- American Society for Metabolic and Bariatric Surgery. [Accessed March 2010];Laproscopic adjustable gastric banding. Available at: http://www.asbs.org/html/patients/bypass.html.
-
- Poves I, Cabrera M, Maristany C, Coma A, Ballesta-Lopez C. Gastrointestinal quality of life after laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2006;16:19–23. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
