

The influence of HAART on the efficacy and safety of pegylated interferon and ribavirin therapy for the treatment of chronic HCV infection in HIV-positive Individuals
- PMID: 20452894
- PMCID: PMC3352215
- DOI: 10.1186/2047-783x-15-3-102
The influence of HAART on the efficacy and safety of pegylated interferon and ribavirin therapy for the treatment of chronic HCV infection in HIV-positive Individuals
Abstract
Objective: This study was performed to investigate the impact of HAART versus no HAART and nucleoside free versus nucleoside containing HAART on the efficacy and safety of pegylated interferon and ribavirin therapy for the treatment of chronic HCV infection in HIV/HCV co-infected patients. In addition a control group of HCV mono-infected patients undergoing anti-HCV therapy was evaluated.
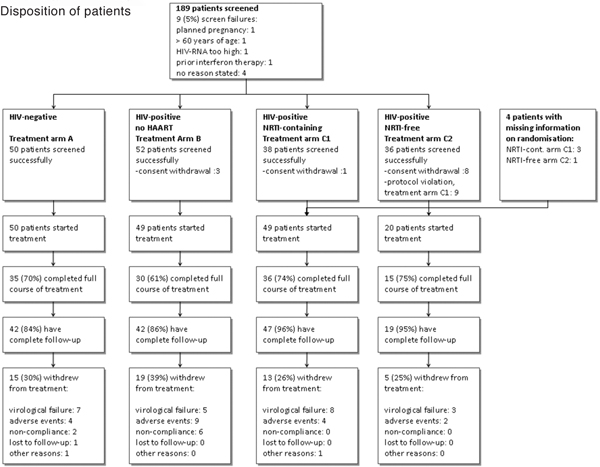
Methods: Multicenter, partially randomized, controlled clinical trial. HIV-negative and -positive patients with chronic HCV infection were treated with pegylated interferon alfa-2a and ribavirin (800 - 1200 mg/day) for 24 - 48 weeks in one of four treatment arms: HIV-negative (A), HIV-positive without HAART (B) and HIV-positive on HAART (C). Patients within arm C were randomized to receive open label either a nucleoside containing (C1) or a nucleoside free HAART (C2).
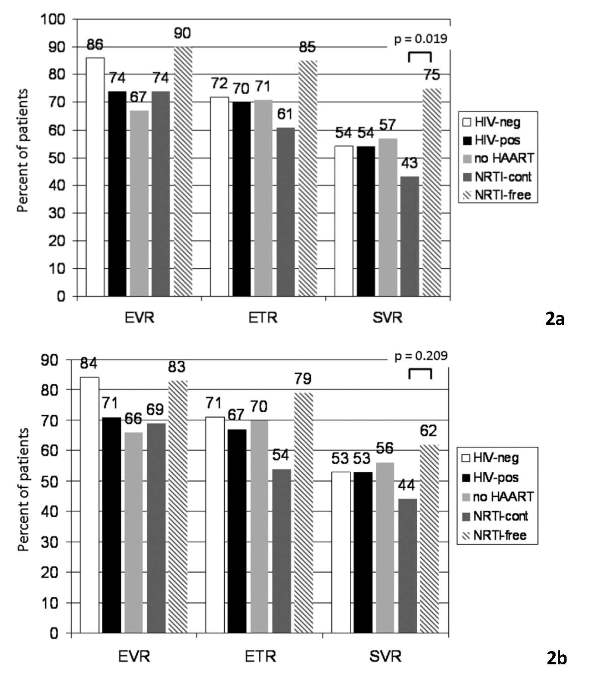
Results: 168 patients were available for analysis. By intent-to-treat analysis similar sustained virological response rates (SVR, negative HCV-RNA 24 weeks after the end of therapy) were observed comparing HIV-negative and -positive patients (54% vs. 54%, p = 1.000). Among HIV-positive patients SVR rates were similar between patients off and on HAART (57% vs. 52%, p = 0.708). Higher SVR rates were observed in patients on a nucleoside free HAART compared to patients on a nucleoside containing HAART, though confounding could not be ruled out and in the intent-to-treat analysis the difference was not statistically significant (64% vs. 46%, p = 0.209).
Conclusions: Similar response rates for HCV therapy can be achieved in HIV-positive and -negative patients. Patients on nucleoside free HAART reached at least equal rates of sustained virological response compared to patients on standard HAART.
Figures
References
-
- Soriano V, Mocroft A, Rockstroh J, Ledergerber B, Knysz B, Chaplinskas S, Peters L, Karlsson A, Katlama C, Toro C, Kupfer B, Vogel M, Lundgren J. Spontaneous viral clearance, viral load, and genotype distribution of hepatitis C virus (HCV) in HIV-infected patients with anti-HCV antibodies in Europe. J Infect Dis. 2008;198:1337–1344. doi: 10.1086/592171. - DOI - PubMed
-
- Rockstroh JK, Mocroft A, Soriano V, Tural C, Losso MH, Horban A, Kirk O, Phillips A, Ledergerber B, Lundgren J. Influence of hepatitis C virus infection on HIV-1 disease progression and response to highly active antiretroviral therapy. J Infect Dis. 2005;192:992–1002. doi: 10.1086/432762. - DOI - PubMed
-
- Rosenthal E, Pialoux G, Bernard N, Pradier C, Rey D, Bentata M, Michelet C, Pol S, Perronne C, Cacoub P. Liver-related mortality in human-immunodeficiencyvirus-infected patients between 1995 and 2003 in the French GERMIVIC Joint Study Group Network (MORTAVIC 2003 Study) J Viral Hepat. 2007;14:183–188. doi: 10.1111/j.1365-2893.2006.00791.x. - DOI - PubMed
-
- Martin-Carbonero L, Benhamou Y, Puoti M, Berenguer J, Mallolas J, Quereda C, Arizcorreta A, Gonzalez A, Rockstroh J, Asensi V, Miralles P, Laguno M, Moreno L, Giron JA, Vogel M, Garcia-Samaniego J, Nunez M, Romero M, Moreno S, de la Cruz JJ, Soriano V. Incidence and predictors of severe liver fibrosis in human immunodeficiency virus-infected patients with chronic hepatitis C: a European collaborative study. Clin Infect Dis. 2004;38:128–133. doi: 10.1086/380130. - DOI - PubMed
-
- Berenguer J, Alvarez-Pellicer J, Martin PM, Lopez-Aldeguer J, Von-Wichmann MA, Quereda C, Mallolas J, Sanz J, Tural C, Bellon JM, Gonzalez-Garcia J. Sustained virological response to interferon plus ribavirin reduces liver-related complications and mortality in patients coinfected with human immunodeficiency virus and hepatitis C virus. Hepatology. 2009;50:407–413. doi: 10.1002/hep.23020. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
