

Relation between time from myocardial infarction to enrolment and patient outcomes in the Multicenter UnSustained Tachycardia Trial
- PMID: 20452992
- PMCID: PMC2910601
- DOI: 10.1093/europace/euq116
Relation between time from myocardial infarction to enrolment and patient outcomes in the Multicenter UnSustained Tachycardia Trial
Abstract
Aims: We sought to assess the relation between time from myocardial infarction (MI) to enrolment and patient outcomes and to examine the association between these outcomes and implantable cardioverter defibrillator (ICD) therapy.
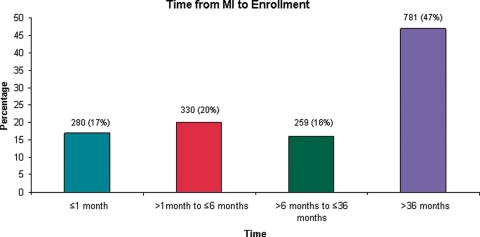
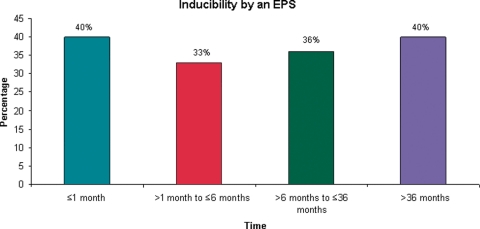
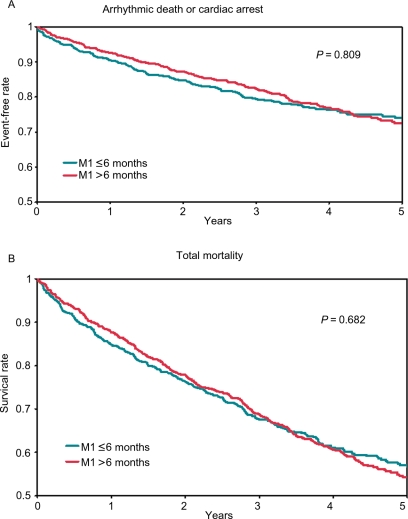
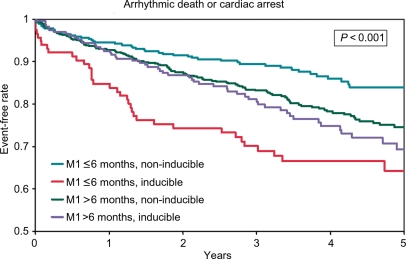
Methods and results: We analysed the Multicenter UnSustained Tachycardia Trial database (n = 1650). In examining all endpoints, Cox proportional hazards models were used to adjust for potential confounders. There was no significant association between time from MI to enrolment and any of the outcomes (P > 0.1). Inducibility by an electrophysiology study (EPS) was associated with a higher risk of arrhythmic death or cardiac arrest [adjusted hazard ratio (HR) 2.51; 95% confidence interval (CI) 1.64-3.84] and all-cause death (adjusted HR 1.45; 95% CI 1.04-2.03) only in patients who had an MI <or=6 months prior to enrolment. ICD therapy was associated with improved survival in patients who had an MI <or=6 months (adjusted HR 0.35; 95% CI 0.17-0.74) and >6 months before enrolment (adjusted HR 0.34; 95% CI 0.21-0.54).
Conclusion: The risk of arrhythmic death or cardiac arrest and all-cause death did not vary as a function of time from the most recent MI to enrolment. Inducibility by an EPS was associated with worse outcomes only in patients with an MI <or=6 months prior to enrolment. Although ICD therapy was associated with improved survival regardless of the time from MI to enrolment, this finding needs to be verified by a randomized clinical trial.
Figures
Comment in
-
Timing of implantation of cardioverter-defibrillator after acute myocardial infarction.Europace. 2010 Aug;12(8):1057-8. doi: 10.1093/europace/euq151. Epub 2010 May 24. Europace. 2010. PMID: 20501470 No abstract available.
References
-
- Huikuri HV, Tapanainen JM, Lindgren K, Raatikainen P, Mäkikallio TH, Juhani Airaksinen KE, et al. Prediction of sudden cardiac death after myocardial infarction in the beta-blocking era. J Am Coll Cardiol. 2003;42:652–8. doi:10.1016/S0735-1097(03)00783-6. - DOI - PubMed
-
- Solomon S, Zelenkofske S, McMurray JJ, Finn PV, Velazquez E, Ertl G, et al. Sudden death in patients with myocardial infarction and left ventricular dysfunction, heart failure, or both. N Engl J Med. 2005;352:2581–8. doi:10.1056/NEJMoa043938. - DOI - PubMed
-
- Moss AJ, Hall WJ, Cannom DS, Daubert JP, Higgins SL, Klein H, et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmias. N Engl J Med. 1996;335:1933–40. doi:10.1056/NEJM199612263352601. - DOI - PubMed
-
- Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN, Hafley G. A randomized study of the prevention of sudden death in patients with coronary artery disease. N Engl J Med. 1999;341:1882–90. doi:10.1056/NEJM199912163412503. - DOI - PubMed
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–83. doi:10.1056/NEJMoa013474. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
