

Risk of colon cancer and coffee, tea, and sugar-sweetened soft drink intake: pooled analysis of prospective cohort studies
- PMID: 20453203
- PMCID: PMC2879415
- DOI: 10.1093/jnci/djq107
Risk of colon cancer and coffee, tea, and sugar-sweetened soft drink intake: pooled analysis of prospective cohort studies
Abstract
Background: The relationships between coffee, tea, and sugar-sweetened carbonated soft drink consumption and colon cancer risk remain unresolved.
Methods: We investigated prospectively the association between coffee, tea, and sugar-sweetened carbonated soft drink consumption and colon cancer risk in a pooled analysis of primary data from 13 cohort studies. Among 731 441 participants followed for up to 6-20 years, 5604 incident colon cancer case patients were identified. Study-specific relative risks (RRs) and 95% confidence intervals (CIs) were estimated using Cox proportional hazards models and then pooled using a random-effects model. All statistical tests were two-sided.
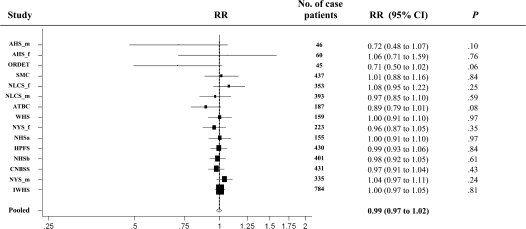
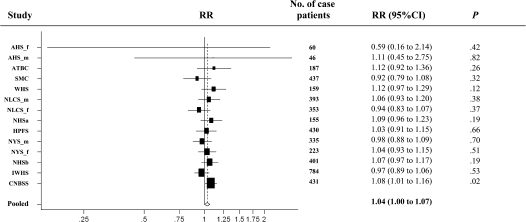
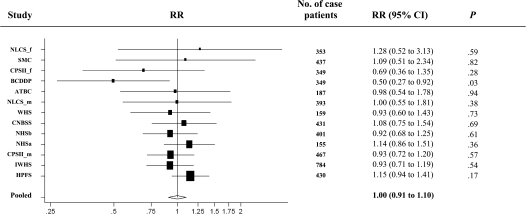
Results: Compared with nonconsumers, the pooled multivariable relative risks were 1.07 (95% CI = 0.89 to 1.30, P(trend) = .68) for coffee consumption greater than 1400 g/d (about six 8-oz cups) and 1.28 (95% CI = 1.02 to 1.61, P(trend) = .01) for tea consumption greater than 900 g/d (about four 8-oz cups). For sugar-sweetened carbonated soft drink consumption, the pooled multivariable relative risk comparing consumption greater than 550 g/d (about 18 oz) to nonconsumers was 0.94 (95% CI = 0.66 to 1.32, P(trend) = .91). No statistically significant between-studies heterogeneity was observed for the highest category of each beverage consumed (P > .20). The observed associations did not differ by sex, smoking status, alcohol consumption, body mass index, physical activity, or tumor site (P > .05).
Conclusions: Drinking coffee or sugar-sweetened carbonated soft drinks was not associated with colon cancer risk. However, a modest positive association with higher tea consumption is possible and requires further study.
Figures
Comment in
-
Coffee, tea, what beverage for me? Associations between beverage intake and colorectal neoplasia risk.J Natl Cancer Inst. 2010 Jun 2;102(11):749-51. doi: 10.1093/jnci/djq158. Epub 2010 May 7. J Natl Cancer Inst. 2010. PMID: 20453202 No abstract available.
References
-
- Ferlay J, Bray F, Pisani P, Parkin D. GLOBOCAN 2002: Cancer Incidence, Mortality and Prevalence Worldwide. IARC CancerBase No. 5 version 2.0. Lyon, France: IARC Press; 2004.
-
- Word Cancer Research Fund. Food, Nutrition and the Prevention of Cancer: A Global Perspective. Washington, DC: American Institute for Cancer Research; 2007. American Institute for Cancer Research Expert Panel. - PubMed
-
- Potter JD. Nutrition and colorectal cancer. Cancer Causes Control. 1996;7(1):127–146. - PubMed
-
- Higdon JV, Frei B. Tea catechins and polyphenols: health effects, metabolism, and antioxidant functions. Crit Rev Food Sci Nutr. 2003;43(1):89–143. - PubMed
