

Randomized controlled trial of trained patient-nominated treatment supporters providing partial directly observed antiretroviral therapy
- PMID: 20453627
- PMCID: PMC2888722
- DOI: 10.1097/QAD.0b013e328339e20e
Randomized controlled trial of trained patient-nominated treatment supporters providing partial directly observed antiretroviral therapy
Abstract
Background: Directly observed therapy (DOT) for antiretroviral therapy (ART) may improve adherence, but there are limited data on its clinical effectiveness.
Methods: Adult patients initiating ART in a public clinic in Cape Town, South Africa, were randomized to treatment-supporter DOT-ART or self-administered ART. DOT-ART patients and supporters received baseline and follow-up training and monitoring. The primary endpoints were the proportions of patients with HIV viral load less than 400 copies/ml and change in CD4 cell counts at 12 and 24 months.
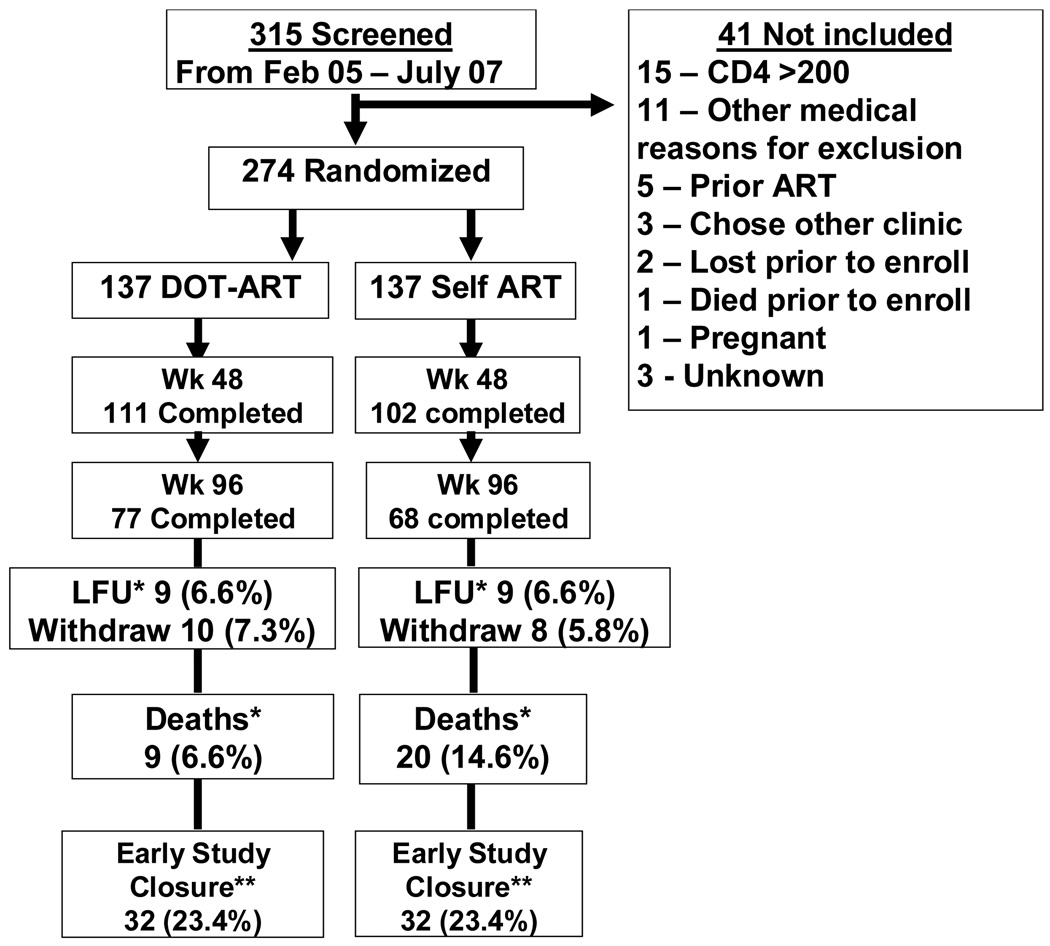
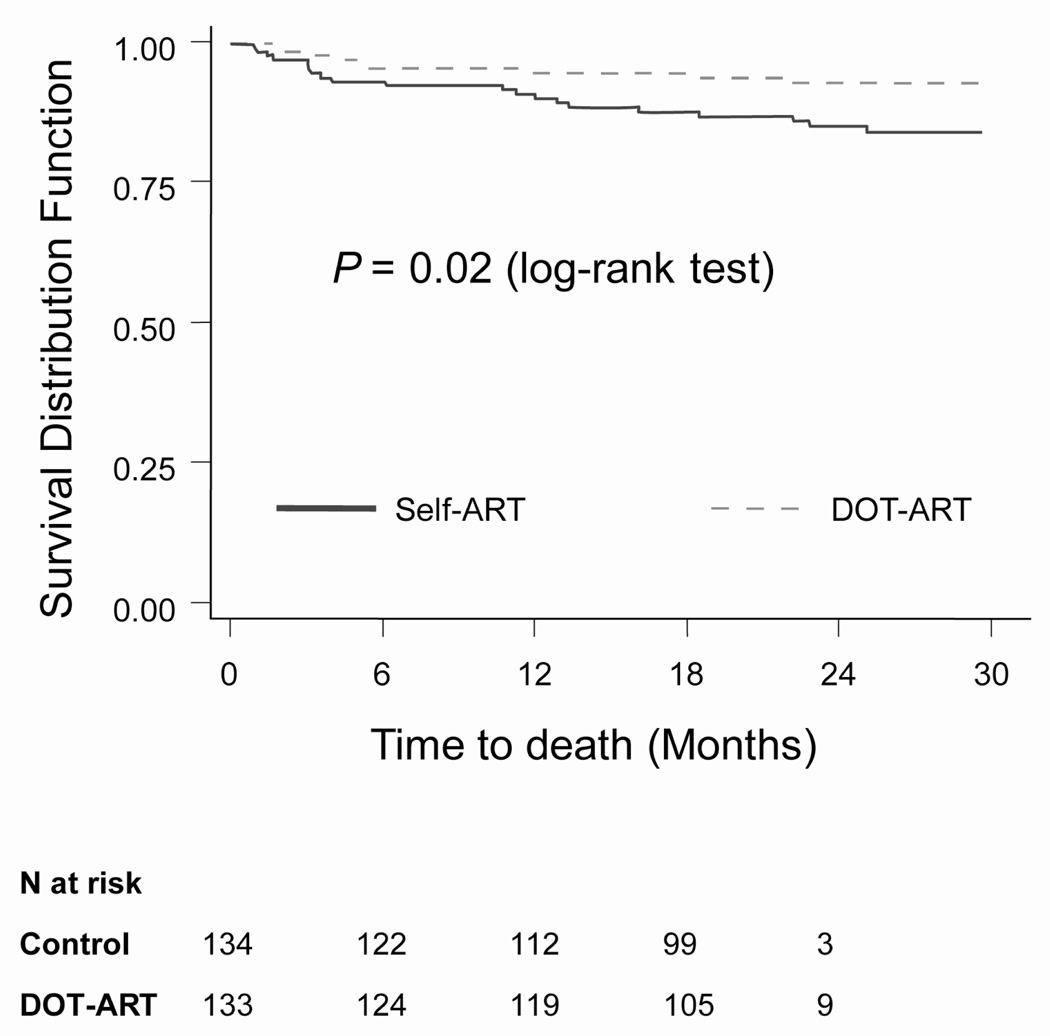
Results: Two hundred and seventy-four patients enrolled (137 in each arm) and baseline characteristics were similar for both arms. The study was stopped early for futility by an independent Data and Safety Monitoring Board. In an intention-to-treat analysis, the proportions of patients with viral load less than 400 copies/ml at 12 months were 72.8% in the DOT-ART arm and 68.4% in the Self-ART arm (P = 0.42). DOT-ART patients had greater median CD4 cell count (cells/microl) increases at 6 months [148 (IQR 84-222) vs. 111 (IQR 44-196) P = 0.02] but similar results at all other time-points. Survival was significantly better in the DOT-ART arm (9 deaths, 6.6%) than in the Self-ART arm (20 deaths, 14.6%; log-rank P = 0.02). In Cox regression analysis, mortality was independently associated with study arm [DOT vs. self-ART; HR 0.38, 95% confidence interval (CI) 0.17-0.86].
Conclusion: DOT-ART showed no effect on virologic outcomes but was associated with greater CD4 cell count increases at 6-month follow-up. Survival was significantly better for DOT-ART compared to Self-ART, but this was not explained by improved virologic or immunologic outcomes.
Figures
References
-
- Paterson DL, Swindells S, Mohr J, Brester M, Vergis EN, Squier C, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000 Jul 4;133(1):21–30. - PubMed
-
- Nachega JB, Hislop M, Dowdy DW, Chaisson RE, Regensberg L, Maartens G. Adherence to nonnucleoside reverse transcriptase inhibitor-based HIV therapy and virologic outcomes. Ann Intern Med. 2007;146:564–573. - PubMed
-
- Harrigan PR, Hogg RS, Dong WW, Yip B, Wynhoven B, Woodward J, et al. Predictors of HIV drug-resistance mutations in a large antiretroviral-naive cohort initiating triple antiretroviral therapy. J Infect Dis. 2005 Feb 1;191(3):339–347. - PubMed
-
- Oyugi JH, Byakika-Tusiime J, Ragland K, Laeyendecker O, Mugerwa R, Kityo C, et al. Treatment interruptions predict resistance in HIV-positive individuals purchasing fixed-dose combination antiretroviral therapy in Kampala, Uganda. AIDS. 2007 May 11;21(8):965–971. - PubMed
-
- Bangsberg DR, Perry S, Charlebois ED, Clark RA, Roberston M, Zolopa AR, et al. Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. AIDS. 2001 Jun 15;15(9):1181–1183. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
