

Surgical versus nonoperative treatment for lumbar spinal stenosis four-year results of the Spine Patient Outcomes Research Trial
- PMID: 20453723
- PMCID: PMC3392200
- DOI: 10.1097/BRS.0b013e3181e0f04d
Surgical versus nonoperative treatment for lumbar spinal stenosis four-year results of the Spine Patient Outcomes Research Trial
Abstract
Study design: Randomized trial and concurrent observational cohort study.
Objective: To compare 4 year outcomes of surgery to nonoperative care for spinal stenosis.
Summary of background data: Surgery for spinal stenosis has been shown to be more effective compared to nonoperative treatment over 2 years, but longer-term data have not been analyzed.
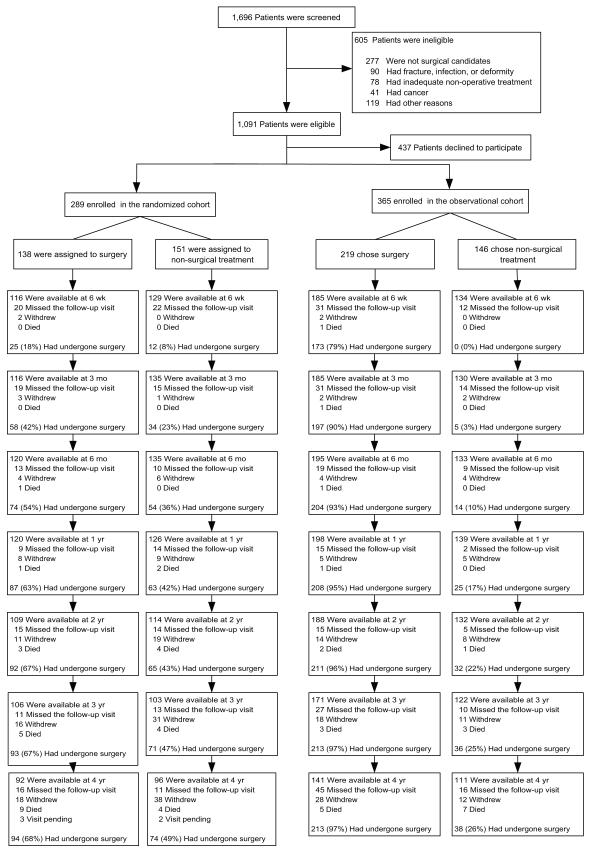
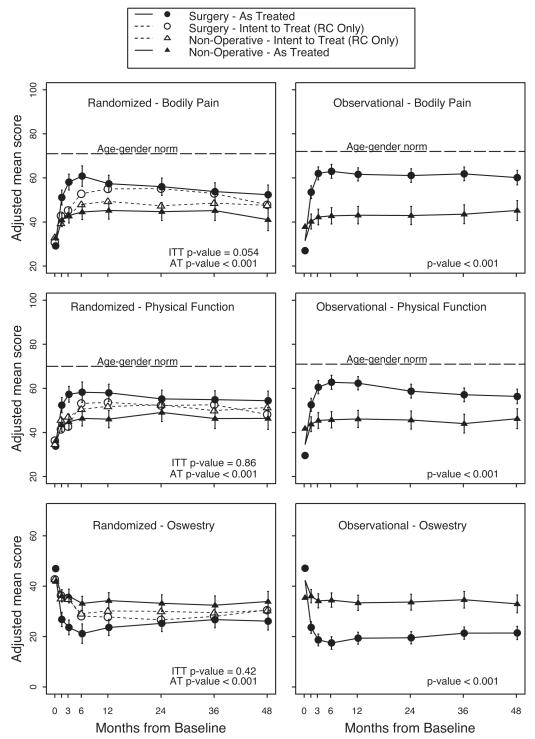
Methods: Surgical candidates from 13 centers in 11 US states with at least 12 weeks of symptoms and confirmatory imaging were enrolled in a randomized cohort (RC) or observational cohort (OC). Treatment was standard decompressive laminectomy or standard nonoperative care. Primary outcomes were SF-36 bodily pain (BP) and physical function scales and the modified Oswestry Disability index assessed at 6 weeks, 3 months, 6 months, and yearly up to 4 years.
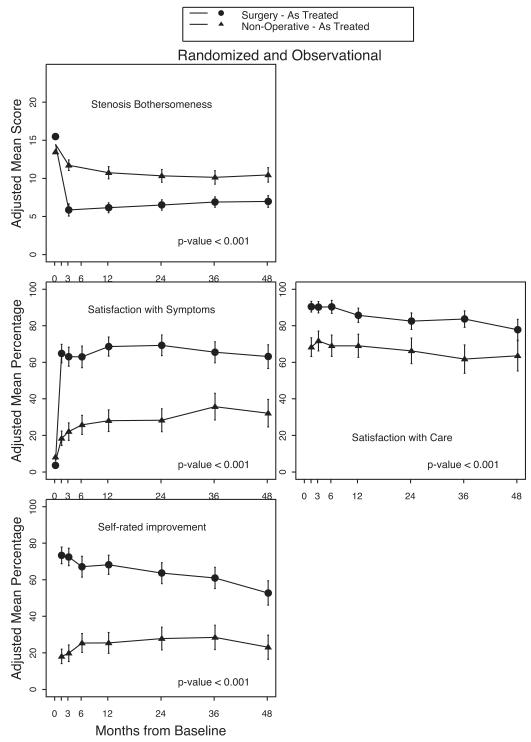
Results: A total of 289 patients enrolled in the RC and 365 patients enrolled in the OC. An as-treated analysis combining the RC and OC and adjusting for potential confounders found that the clinically significant advantages for surgery previously reported were maintained through 4 years, with treatment effects (defined as mean change in surgery group minus mean change in nonoperative group) for bodily pain 12.6 (95% confidence interval [CI], 8.5-16.7); physical function 8.6 (95% CI, 4.6-12.6); and Oswestry Disability index -9.4 (95% CI, -12.6 to -6.2). Early advantages for surgical treatment for secondary measures such as bothersomeness, satisfaction with symptoms, and self-rated progress were also maintained.
Conclusion: Patients with symptomatic spinal stenosis treated surgically compared to those treated nonoperatively maintain substantially greater improvement in pain and function through 4 years.
Trial registration: ClinicalTrials.gov NCT00000411.
References
-
- Malmivaara A, Slatis P, Heliovaara M, et al. Surgical or nonoperative treatment for lumbar spinal stenosis?: a randomized controlled trial. Spine. 2007;32:1–8. - PubMed
-
- Atlas SJ, Deyo RA, Keller RB, et al. The Maine Lumbar Spine Study, Part III. 1-year outcomes of surgical and nonsurgical management of lumbar spinal stenosis. Spine. 1996;21:1787–94. discussion 94-5. - PubMed
-
- Bridwell KH, Sedgewick TA, O’Brien MF, et al. The role of fusion and instrumentation in the treatment of degenerative spondylolisthesis with spinal stenosis. J Spinal Disord. 1993;6:461–72. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
