

Anatomy of the epidemiological literature on the 2003 SARS outbreaks in Hong Kong and Toronto: a time-stratified review
- PMID: 20454570
- PMCID: PMC2864302
- DOI: 10.1371/journal.pmed.1000272
Anatomy of the epidemiological literature on the 2003 SARS outbreaks in Hong Kong and Toronto: a time-stratified review
Abstract
Background: Outbreaks of emerging infectious diseases, especially those of a global nature, require rapid epidemiological analysis and information dissemination. The final products of those activities usually comprise internal memoranda and briefs within public health authorities and original research published in peer-reviewed journals. Using the 2003 severe acute respiratory syndrome (SARS) epidemic as an example, we conducted a comprehensive time-stratified review of the published literature to describe the different types of epidemiological outputs.
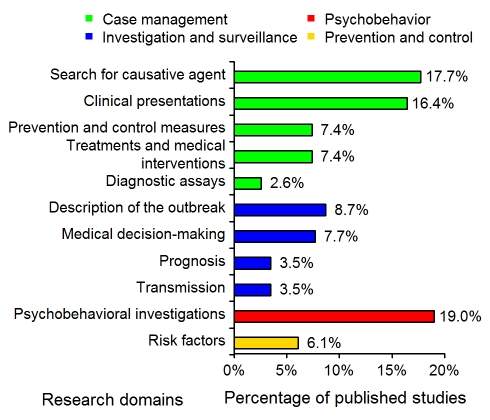
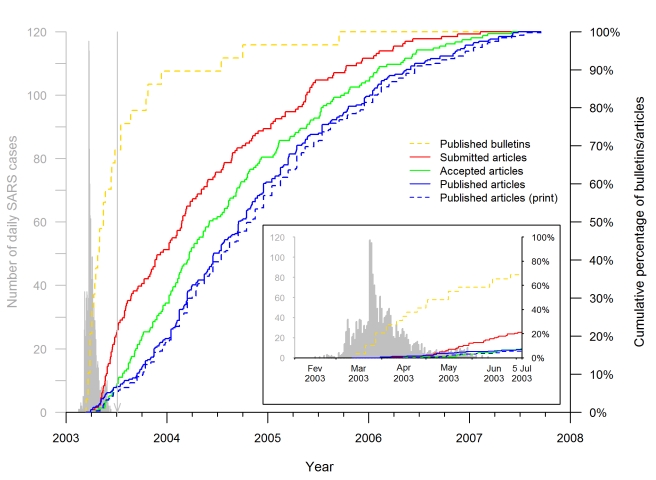
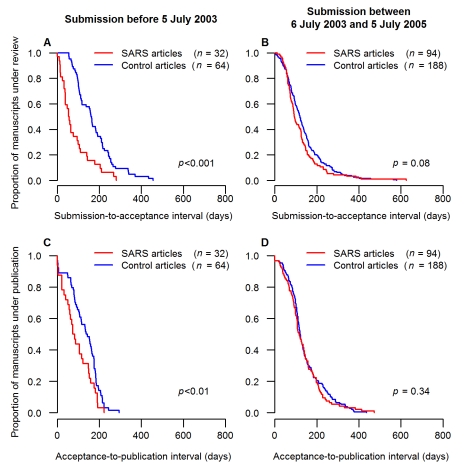
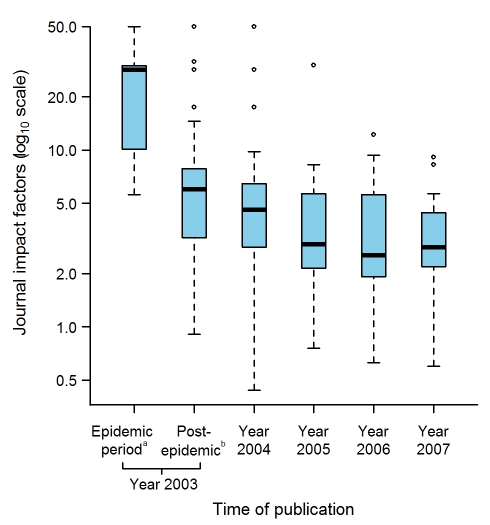
Methods and findings: We identified and analyzed all published articles on the epidemiology of the SARS outbreak in Hong Kong or Toronto. The analysis was stratified by study design, research domain, data collection, and analytical technique. We compared the SARS-case and matched-control non-SARS articles published according to the timeline of submission, acceptance, and publication. The impact factors of the publishing journals were examined according to the time of publication of SARS articles, and the numbers of citations received by SARS-case and matched-control articles submitted during and after the epidemic were compared. Descriptive, analytical, theoretical, and experimental epidemiology concerned, respectively, 54%, 30%, 11%, and 6% of the studies. Only 22% of the studies were submitted, 8% accepted, and 7% published during the epidemic. The submission-to-acceptance and acceptance-to-publication intervals of the SARS articles submitted during the epidemic period were significantly shorter than the corresponding intervals of matched-control non-SARS articles published in the same journal issues (p<0.001 and p<0.01, respectively). The differences of median submission-to-acceptance intervals and median acceptance-to-publication intervals between SARS articles and their corresponding control articles were 106.5 d (95% confidence interval [CI] 55.0-140.1) and 63.5 d (95% CI 18.0-94.1), respectively. The median numbers of citations of the SARS articles submitted during the epidemic and over the 2 y thereafter were 17 (interquartile range [IQR] 8.0-52.0) and 8 (IQR 3.2-21.8), respectively, significantly higher than the median numbers of control article citations (15, IQR 8.5-16.5, p<0.05, and 7, IQR 3.0-12.0, p<0.01, respectively).
Conclusions: A majority of the epidemiological articles on SARS were submitted after the epidemic had ended, although the corresponding studies had relevance to public health authorities during the epidemic. To minimize the lag between research and the exigency of public health practice in the future, researchers should consider adopting common, predefined protocols and ready-to-use instruments to improve timeliness, and thus, relevance, in addition to standardizing comparability across studies. To facilitate information dissemination, journal managers should reengineer their fast-track channels, which should be adapted to the purpose of an emerging outbreak, taking into account the requirement of high standards of quality for scientific journals and competition with other online resources.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
Journals, academics, and pandemics.PLoS Med. 2010 May 25;7(5):e1000282. doi: 10.1371/journal.pmed.1000282. PLoS Med. 2010. PMID: 20520802 Free PMC article.
References
-
- Connolly MA. Communicable disease control in emergencies – a field manual. Geneva: World Health Organization. 2005. Available: http://www.who.int/infectious-disease-news/IDdocs/whocds200527/ISBN_9241.... Accessed 16 May 2008.
-
- Heymann DL, Rodier GR. Hot spots in a wired world: WHO surveillance of emerging and re-emerging infectious diseases. Lancet Infect Dis. 2001;1:345–353. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
