

Mineralocorticoid deficiency and treatment in congenital adrenal hyperplasia
- PMID: 20454572
- PMCID: PMC2864445
- DOI: 10.1155/2010/656925
Mineralocorticoid deficiency and treatment in congenital adrenal hyperplasia
Abstract
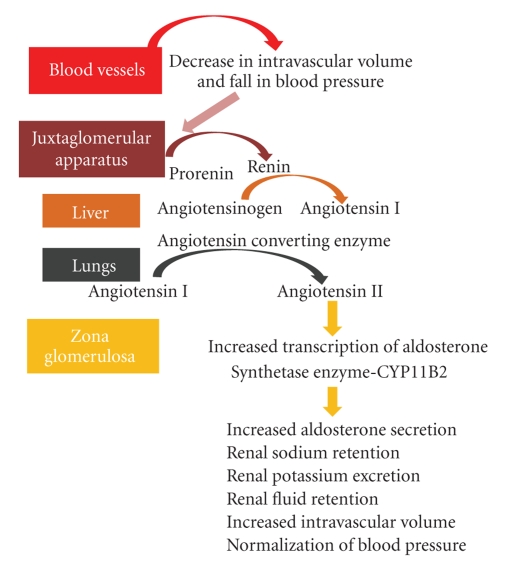
Approximately 75%-80% of patients with Congenital Adrenal Hyperplasia (CAH) fail to synthesize sufficient mineralocorticoids to maintain salt and water balance. In most instances genotype can predict mineralocorticoid deficiency in CAH. Early recognition and replacement with 9alpha-fludrocortisone and salt supplements will prevent development of potentially lethal salt losing crises. In infancy a relative state of aldosterone resistance exists and replacement dose of 9alpha-fludrocortisone based on body surface area is higher during infancy compared to childhood and adults. Salt supplementation is generally not required after weaning is started. Regular monitoring of blood pressure and measurements of plasma electrolytes and renin are required to prevent complications of under or over dosage.
Figures
References
-
- White PC, Speiser PW. Congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Endocrinology Reviews. 2000;21(3):245–291. - PubMed
-
- Rhéaume E, Simard J, Morel Y, et al. Congenital adrenal hyperplasia due to point mutations in the type II 3 β-hydroxysteroid dehydrogenase gene. Nature Genetics. 1992;1(4):239–245. - PubMed
-
- Jääskeläinen J, Levo A, Voutilainen R, Partanen J. Population-wide evaluation of disease manifestation in relation to molecular genotype in steroid 21-hydroxylase (CYP21) deficiency: good correlation in a well defined population. Journal of Clinical Endocrinology & Metabolism. 1997;82(10):3293–3297. - PubMed
-
- Krone N, Braun A, Roscher AA, Knorr D, Schwarz HP. Predicting phenotype in steroid 21-hydroxylase deficiency? Comprehensive genotyping in 155 unrelated, well defined patients from southern Germany. Journal of Clinical Endocrinology & Metabolism. 2000;85(3):1059–1065. - PubMed
LinkOut - more resources
Full Text Sources
