

Failure to achieve clinical improvement despite graft patency in patients undergoing infrainguinal lower extremity bypass for critical limb ischemia
- PMID: 20456908
- PMCID: PMC5240817
- DOI: 10.1016/j.jvs.2010.01.083
Failure to achieve clinical improvement despite graft patency in patients undergoing infrainguinal lower extremity bypass for critical limb ischemia
Abstract
Objective: Studies of infrainguinal lower extremity bypass for critical limb ischemia (CLI) have traditionally emphasized outcomes of patency, limb salvage, and death. Because functional outcomes are equally important, our objectives were to describe the proportion of CLI patients who did not achieve symptomatic improvement 1 year after bypass, despite having patent grafts, and identify preoperative factors associated with this outcome.
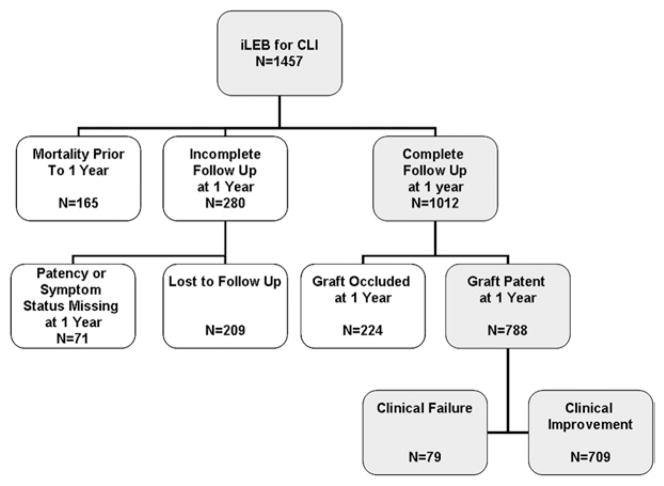
Methods: The prospectively collected Vascular Study Group of Northern New England database was used to identify all patients with elective infrainguinal lower extremity bypass for CLI (2003 to 2007) for whom long-term follow-up data were available. The primary composite study end point was clinical failure at 1 year after bypass, defined as amputation or persistent or worsened ischemic symptoms (rest pain or tissue loss), despite a patent graft. Variables identified on univariate screening (inclusion threshold, P < .20) were included in a multivariable logistic regression model to identify independent predictors.
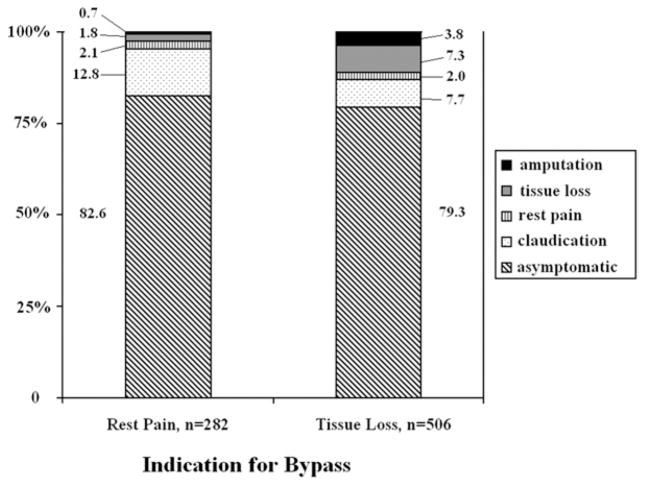
Results: Long-term follow-up data were available for 1012 patients who underwent infrainguinal bypasses for CLI, of which 788 (78%) remained patent at 1 year. Of these, 79 (10%) met criteria for the composite end point of clinical failure: 21 (2.7%) for major amputations and 58 (7.4%) for persistent rest pain or tissue loss. In multivariable analysis, significant predictors of clinical failure included dialysis dependence (odds ratio [OR], 3.74; 95% confidence interval [CI], 1.84-7.62; P < .001) and preoperative inability to ambulate independently (OR, 2.17; 95% CI, 1.26-3.73; P = .005). A history of coronary artery bypass graft or percutaneous coronary intervention was protective (OR, 0.52; 95% CI, 0.29-0.93; P = .03).
Conclusions: After infrainguinal lower extremity bypass for CLI, 10% of patients with a patent graft did not achieve clinical improvement at 1 year. Preoperative identification of this specific patient subgroup remains challenging. To improve surgical decision making and the overall care of CLI patients, further emphasis needs to be placed on functional outcomes in addition to traditional surgical end points.
Copyright (c) 2010 Society for Vascular Surgery. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
Competition of interest: none. The editors and reviewers of this article have no relevant financial relationships to disclose per the JVS policy that requires reviewers to decline review of any manuscript for which they may have a competition of interest.
Figures
Similar articles
-
Defining utility and predicting outcome of cadaveric lower extremity bypass grafts in patients with critical limb ischemia.J Vasc Surg. 2014 Dec;60(6):1554-64. doi: 10.1016/j.jvs.2014.06.009. Epub 2014 Jul 16. J Vasc Surg. 2014. PMID: 25043889 Free PMC article.
-
Predictors of major amputation despite patent bypass grafts.J Vasc Surg. 2016 May;63(5):1279-88. doi: 10.1016/j.jvs.2015.10.101. Epub 2016 Feb 6. J Vasc Surg. 2016. PMID: 26860641 Clinical Trial.
-
Outcomes of infrainguinal bypass determined by age in the Vascular Study Group of New England.J Vasc Surg. 2015 Jul;62(1):83-92. doi: 10.1016/j.jvs.2015.02.020. Epub 2015 May 4. J Vasc Surg. 2015. PMID: 25953015 Free PMC article.
-
End-stage renal disease patients undergoing angioplasty and bypass for critical limb ischemia have worse outcomes compared to non-ESRD patients: Systematic review and meta-analysis.Catheter Cardiovasc Interv. 2021 Aug 1;98(2):297-307. doi: 10.1002/ccd.29688. Epub 2021 Apr 6. Catheter Cardiovasc Interv. 2021. PMID: 33825331
-
Understanding objective performance goals for critical limb ischemia trials.Semin Vasc Surg. 2010 Sep;23(3):129-37. doi: 10.1053/j.semvascsurg.2010.06.001. Semin Vasc Surg. 2010. PMID: 20826289 Review.
Cited by
-
Defining utility and predicting outcome of cadaveric lower extremity bypass grafts in patients with critical limb ischemia.J Vasc Surg. 2014 Dec;60(6):1554-64. doi: 10.1016/j.jvs.2014.06.009. Epub 2014 Jul 16. J Vasc Surg. 2014. PMID: 25043889 Free PMC article.
-
Impact of Chronic Renal Failure on Safety and Effectiveness of Paclitaxel-Eluting Stents for Femoropopliteal Artery Disease: Subgroup Analysis from Zilver PTX Post-Market Surveillance Study in Japan.Cardiovasc Intervent Radiol. 2017 Nov;40(11):1669-1677. doi: 10.1007/s00270-017-1673-6. Epub 2017 May 9. Cardiovasc Intervent Radiol. 2017. PMID: 28488101 Free PMC article.
-
Critical limb ischemia.Curr Treat Options Cardiovasc Med. 2010 Jun;12(3):214-29. doi: 10.1007/s11936-010-0076-7. Epub 2010 Apr 14. Curr Treat Options Cardiovasc Med. 2010. PMID: 20461120 Free PMC article.
-
Long-term results after femoral thrombendarterectomy combined with simultaneous endovascular intervention in intermittent claudication and critical ischemia.SAGE Open Med. 2020 Jan 15;8:2050312119900860. doi: 10.1177/2050312119900860. eCollection 2020. SAGE Open Med. 2020. PMID: 32002182 Free PMC article.
-
The comparative efficacy of angiosome-directed and indirect revascularisation strategies to aid healing of chronic foot wounds in patients with co-morbid diabetes mellitus and critical limb ischaemia: a literature review.J Foot Ankle Res. 2017 Jun 28;10:26. doi: 10.1186/s13047-017-0206-5. eCollection 2017. J Foot Ankle Res. 2017. PMID: 28670345 Free PMC article. Review.
References
-
- Schanzer A, Hevelone N, Owens CD, Belkin M, Bandyk DF, Clowes AW, et al. Technical factors affecting autogenous vein graft failure: observations from a large multicenter trial. J Vasc Surg. 2007;46:1180–90. discussion 90. - PubMed
-
- Robinson WP, 3rd, Owens CD, Nguyen LL, Chong TT, Conte MS, Belkin M. Inferior outcomes of autogenous infrainguinal bypass in Hispanics: an analysis of ethnicity, graft function, and limb salvage. J Vasc Surg. 2009;49:1416–25. - PubMed
-
- Rossi PJ, Skelly CL, Meyerson SL, Bassiouny HS, Katz D, Schwartz LB, et al. Redo infrainguinal bypass: factors predicting patency and limb salvage. Ann Vasc Surg. 2003;17:492–502. - PubMed
-
- Toursarkissian B, D’Ayala M, Stefanidis D, Shireman PK, Harrison A, Schoolfield J, et al. Angiographic scoring of vascular occlusive disease in the diabetic foot: relevance to bypass graft patency and limb salvage. J Vasc Surg. 2002;35:494–500. - PubMed
-
- Owens CD, Ho KJ, Kim S, Schanzer A, Lin J, Matros E, et al. Refinement of survival prediction in patients undergoing lower extremity bypass surgery: stratification by chronic kidney disease classification. J Vasc Surg. 2007;45:944–52. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
