

Viral epidemiologic shift in inflammatory heart disease: the increasing involvement of parvovirus B19 in the myocardium of pediatric cardiac transplant patients
- PMID: 20456978
- PMCID: PMC2902647
- DOI: 10.1016/j.healun.2010.03.003
Viral epidemiologic shift in inflammatory heart disease: the increasing involvement of parvovirus B19 in the myocardium of pediatric cardiac transplant patients
Abstract
Background: Detection of viral genome in rejecting cardiac transplant patients has been reported, with coxsackievirus and adenovirus causing premature graft failure. Recently, parvovirus B19 (PVB19) genome in myocardial samples has been increasingly reported, but its role in cardiac pathology and effect on transplant graft survival are unknown. The objectives of this study were to determine if changes in the viruses identified in the myocardium represent an epidemiologic shift in viral myocardial disease and whether PVB19 adversely affects transplant graft survival.
Methods: From September 2002 to December 2005, nested polymerase chain reaction was used to evaluate endomyocardial biopsy specimens for 99 children (aged 3 weeks-18 years) with heart transplants for the presence of viral genome. Cellular rejection was assessed by histology of specimens. Transplant coronary artery disease (TCAD) was diagnosed by coronary angiography or histopathology.
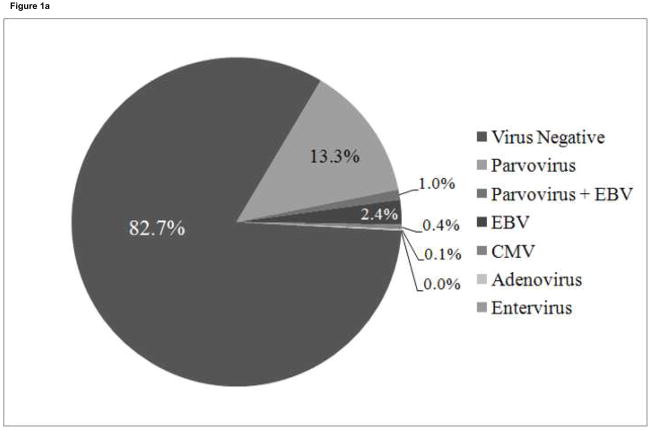
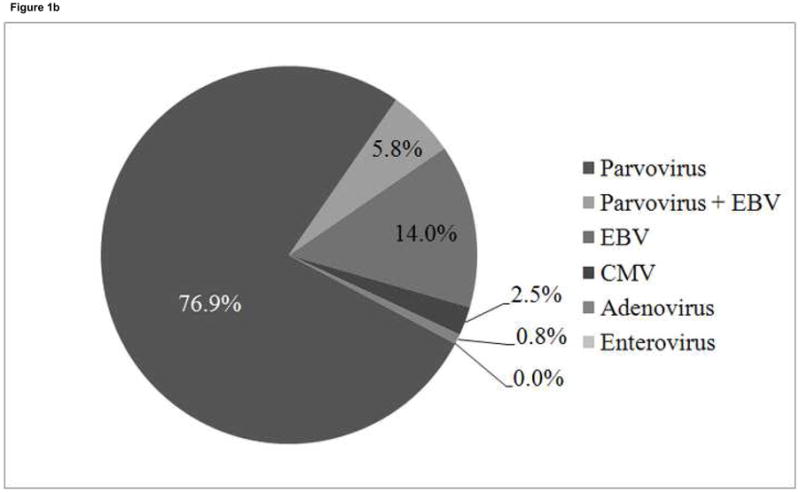
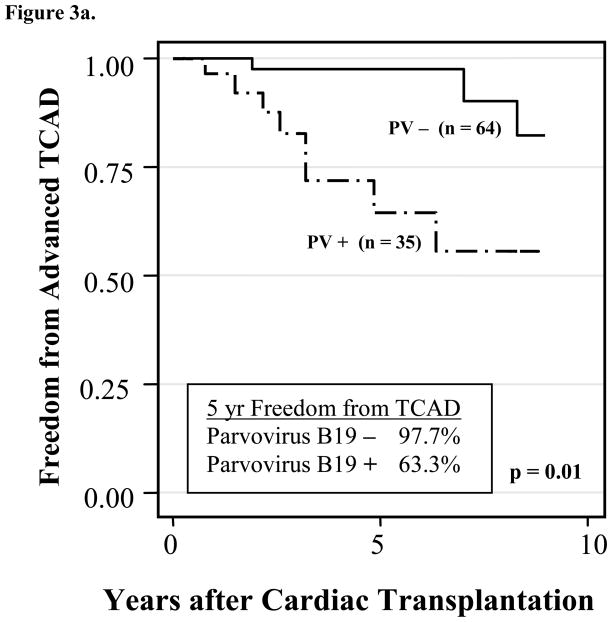
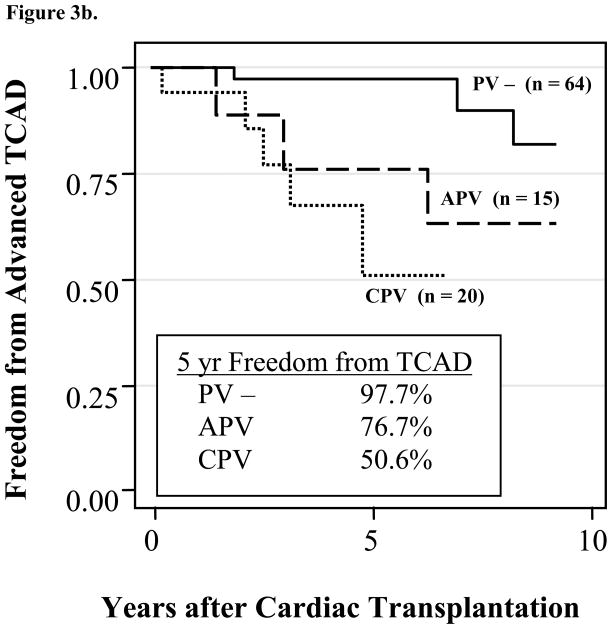
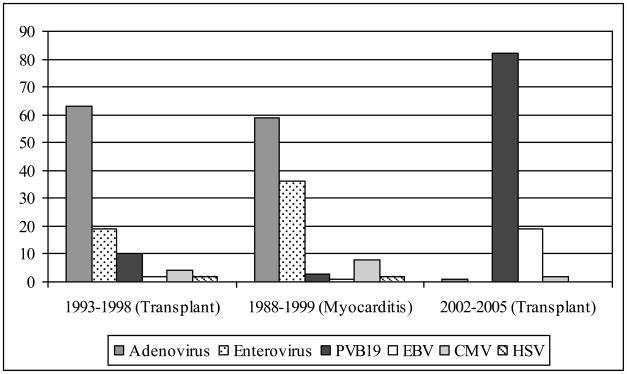
Results: Specimens from 700 biopsies were evaluated from 99 patients; 121 specimens had viral genome, with 100 (82.6%) positive for PVB19, 24 for Epstein-Barr virus (EBV; 7 positive for PVB19 and EBV), 3 for CMV, and 1 for adenovirus. Presence of PVB19 genome did not correlate with rejection score, nor did a higher viral copy number. Early development of advanced TCAD (p < 0.001) occurred in 20 children with persistent PVB19 infection (> 6 months).
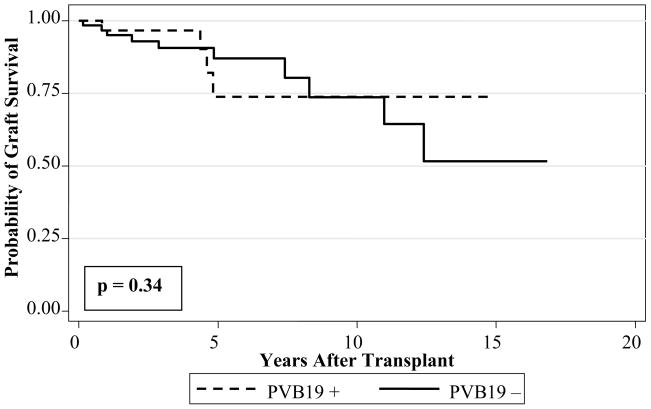
Conclusions: PVB19 is currently the predominant virus detected in heart transplant surveillance biopsy specimens, possibly representing an epidemiologic shift. Cellular rejection does not correlate with the presence or quantity of PVB19 genome in the myocardium, but children with chronic PVB19 infection have increased risk for earlier TCAD, supporting the hypothesis that PVB19 negatively affects graft survival.
Figures
References
-
- Boucek MM, Waltz DA, Edwards LB, et al. Registry of the International Society for Heart and Lung Transplantation: ninth official pediatric heart transplantation report--2006. J Heart Lung Transplant. 2006;25:893–903. - PubMed
-
- Bridges ND, Spray TL, Collins MH, Bowles NE, Towbin JA. Adenovirus infection in the lung results in graft failure after lung transplantation. J Thorac Cardiovasc Surg. 1998;116:617–23. - PubMed
-
- Ramos E, Vincenti F, Lu WX, et al. Retransplantation in patients with graft loss caused by polyoma virus nephropathy. Transplantation. 2004;77:131–3. - PubMed
-
- Kandolf R. Molecular biology of viral heart disease. Herz. 1993;18:238–44. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
