

Multicentre prospective validation of use of the Canadian C-Spine Rule by triage nurses in the emergency department
- PMID: 20457772
- PMCID: PMC2917929
- DOI: 10.1503/cmaj.091430
Multicentre prospective validation of use of the Canadian C-Spine Rule by triage nurses in the emergency department
Abstract
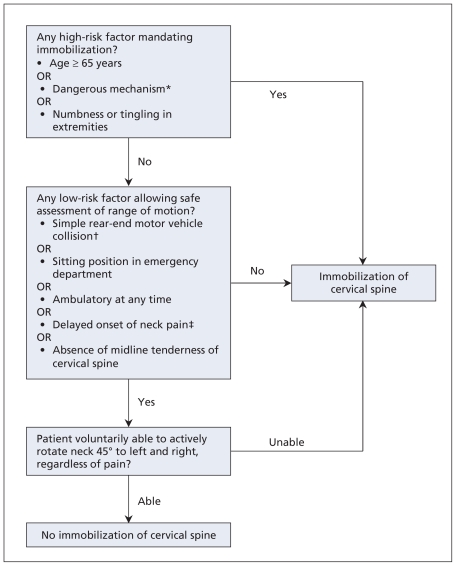
Objectives: The Canadian C-Spine Rule for imaging of the cervical spine was developed for use by physicians. We believe that nurses in the emergency department could use this rule to clinically clear the cervical spine. We prospectively evaluated the accuracy, reliability and acceptability of the Canadian C-Spine Rule when used by nurses.
Methods: We conducted this three-year prospective cohort study in six Canadian emergency departments. The study involved adult trauma patients who were alert and whose condition was stable. We provided two hours of training to 191 triage nurses. The nurses then assessed patients using the Canadian C-Spine Rule, including determination of neck tenderness and range of motion, reapplied immobilization and completed a data form.
Results: Of the 3633 study patients, 42 (1.2%) had clinically important injuries of the cervical spine. The kappa value for interobserver assessments of 498 patients with the Canadian C-Spine Rule was 0.78. We calculated sensitivity of 100.0% (95% confidence interval [CI] 91.0%-100.0%) and specificity of 43.4% (95% CI 42.0%-45.0%) for the Canadian C-Spine Rule as interpreted by the investigators. The nurses classified patients with a sensitivity of 90.2% (95% CI 76.0%-95.0%) and a specificity of 43.9% (95% CI 42.0%-46.0%). Early in the study, nurses failed to identify four cases of injury, despite the presence of clear high-risk factors. None of these patients suffered sequelae, and after retraining there were no further missed cases. We estimated that for 40.7% of patients, the cervical spine could be cleared clinically by nurses. Nurses reported discomfort in applying the Canadian C-Spine Rule in only 4.8% of cases.
Conclusion: Use of the Canadian C-Spine Rule by nurses was accurate, reliable and clinically acceptable. Widespread implementation by nurses throughout Canada and elsewhere would diminish patient discomfort and improve patient flow in overcrowded emergency departments.
Figures
Comment in
-
Incorrectly placed C-spine collar.CMAJ. 2010 Nov 9;182(16):1761. doi: 10.1503/cmaj.110-2121. CMAJ. 2010. PMID: 21059785 Free PMC article. No abstract available.
-
ACP Journal Club. The Canadian C-Spine Rule, used by nurses, accurately identified cervical-spine injury in patients with trauma.Ann Intern Med. 2011 Jan 18;154(2):JC1-13. doi: 10.7326/0003-4819-154-2-201101180-02013. Ann Intern Med. 2011. PMID: 21242355 No abstract available.
References
-
- Pitts SR, Niska RW, Xu J, et al. National Hospital Ambulatory Medical Care Survey: 2006 emergency department summary. Natl Health Stat Rep. 2008;(7):1–38. - PubMed
-
- Chan BT, Schull MJ, Schultz SE. Emergency department services in Ontario 1993–2000. Toronto (ON): Institute for Clinical Evaluative Sciences; 2001.
-
- Schull MJ, Slaughter PM, Redelmeier DA. Urban emergency department overcrowding: defining the problem and eliminating misconceptions. CJEM. 2002;4:76–83. - PubMed
-
- Lindsay P, Bronskill S, Schull MJ, et al. Clinical utilization and outcomes. In: Brown AD, editor. Hospital report 2001: emergency department care. Toronto (ON): Ontario Hospital Association and Government of Ontario; 2001.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical