

Continued high prevalence and adverse clinical impact of human immunodeficiency virus-associated sensory neuropathy in the era of combination antiretroviral therapy: the CHARTER Study
- PMID: 20457954
- PMCID: PMC3924778
- DOI: 10.1001/archneurol.2010.76
Continued high prevalence and adverse clinical impact of human immunodeficiency virus-associated sensory neuropathy in the era of combination antiretroviral therapy: the CHARTER Study
Abstract
Objective: To provide updated estimates of the prevalence and clinical impact of human immunodeficiency virus-associated sensory neuropathy (HIV-SN) and neuropathic pain due to HIV-SN in the combination antiretroviral therapy (CART) era.
Design: Prospective, cross-sectional analysis. Clinical correlates for HIV-SN and neuropathic pain, including age, exposure to CART, CD4 levels, plasma viral load, hepatitis C virus infection, and alcohol use disorders, were evaluated in univariate and multivariate models.
Setting: Six US academic medical centers.
Patients: One thousand five hundred thirty-nine HIV-infected individuals enrolled in the CNS (Central Nervous System) HIV Anti-Retroviral Therapy Effects Research study.
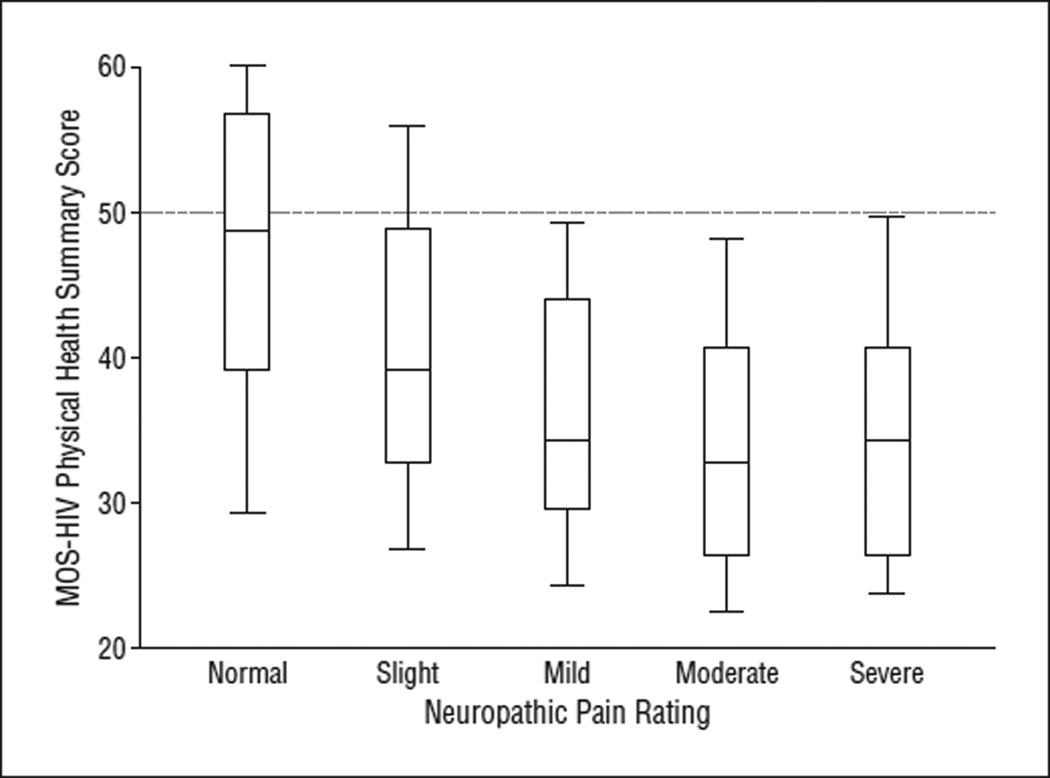
Main outcome measures: The presence of HIV-SN, defined by 1 or more clinical signs (diminished vibration or sharp sensation in the legs and feet; reduced ankle reflexes) in a distal, symmetrical pattern. Neuropathic pain was defined as aching, stabbing, or burning in a similar distribution. The effect on quality of life was assessed with the Medical Outcomes Study HIV Health Survey.
Results: We found HIV-SN in 881 participants. Of these, 38.0% reported neuropathic pain. Neuropathic pain was significantly associated with disability in daily activities, unemployment, and reduced quality of life. Risk factors for HIV-SN after adjustment were advancing age (odds ratio, 2.1 [95% confidence interval, 1.8-2.5] per 10 years), lower CD4 nadir (1.2 [1.1-1.2] per 100-cell decrease), current CART use (1.6 [1.3-2.8]), and past "D-drug" use (specific dideoxynucleoside analogue antiretrovirals) (2.0 [1.3-2.6]). Risk factors for neuropathic pain were past D-drug use and higher CD4 nadir.
Conclusions: Neuropathic pain and HIV-SN remain prevalent, causing substantial disability and reduced quality of life even with successful CART. The clinical correlates of HIV-SN have changed with the evolution of treatment. These findings argue for redoubled efforts to determine HIV-SN pathogenesis and the development of symptomatic and neuroregenerative therapies.
Figures
Comment in
-
Human immunodeficiency virus-associated distal sensory polyneuropathy: still common after many successes.Arch Neurol. 2010 May;67(5):534-5. doi: 10.1001/archneurol.2010.66. Arch Neurol. 2010. PMID: 20457950 No abstract available.
References
-
- Autran B, Carcelain G, Li TS, et al. Positive effects of combined antiretroviral therapy on CD4+T cell homeostasis and function in advanced HIV disease. Science. 1997;277(5322):112–116. - PubMed
-
- Mouton Y, Alfandari S, Valette M, et al. Impact of protease inhibitors on AIDS-defining events and hospitalizations in 10 French AIDS reference centres. AIDS. 1997;11(12):F101–F105. - PubMed
-
- Höke A, Cornblath DR. Peripheral neuropathies in human immunodeficiency virus infection. Suppl Clin Neurophysiol. 2004;57:195–210. - PubMed
-
- Verma S, Estanislao L, Mintz L, Simpson D. Controlling neuropathic pain in HIV. Curr Infect Dis Rep. 2004;6(3):237–242. - PubMed
-
- Ellis RJ, Evans SR, Clifford DB, et al. Neurological AIDS Research Consortium. AIDS Clinical Trials Group Study Teams A5001 and A362. Clinical validation of the NeuroScreen. J Neurovirol. 2005;11(6):503–511. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
