

Effect of systolic blood pressure reduction on hematoma expansion, perihematomal edema, and 3-month outcome among patients with intracerebral hemorrhage: results from the antihypertensive treatment of acute cerebral hemorrhage study
- PMID: 20457956
- PMCID: PMC5562043
- DOI: 10.1001/archneurol.2010.61
Effect of systolic blood pressure reduction on hematoma expansion, perihematomal edema, and 3-month outcome among patients with intracerebral hemorrhage: results from the antihypertensive treatment of acute cerebral hemorrhage study
Abstract
Background: Evidence indicates that systolic blood pressure (SBP) reduction may reduce hematoma expansion in patients with intracerebral hemorrhage (ICH) who are initially seen with acute hypertensive response.
Objective: To explore the relationship between different variables of SBP reduction and hematoma expansion, perihematomal edema, and 3-month outcome among patients with ICH.
Design: Post hoc analysis of a traditional phase 1 dose-escalation multicenter prospective study.
Setting: Emergency departments and intensive care units.
Patients: Patients having ICH with an elevated SBP of at least 170 mm Hg who were seen within 6 hours of symptom onset.
Intervention: Systolic blood pressure reduction using intravenous nicardipine hydrochloride targeting 3 tiers of sequentially escalating SBP reduction goals (170-199, 140-169, or 110-139 mm Hg).
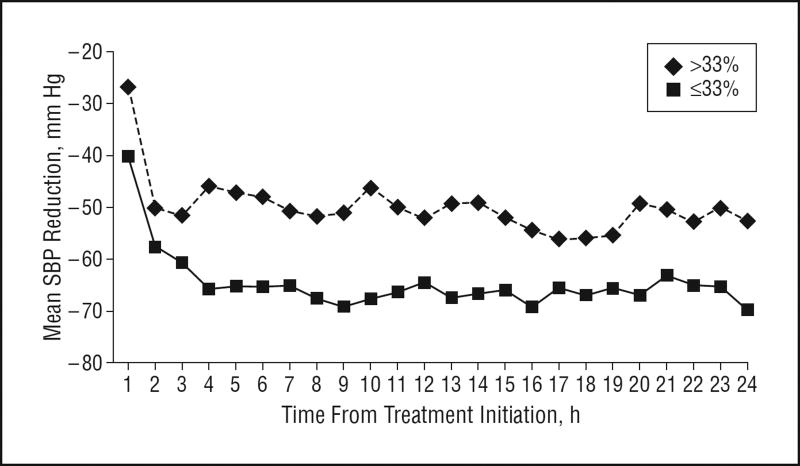
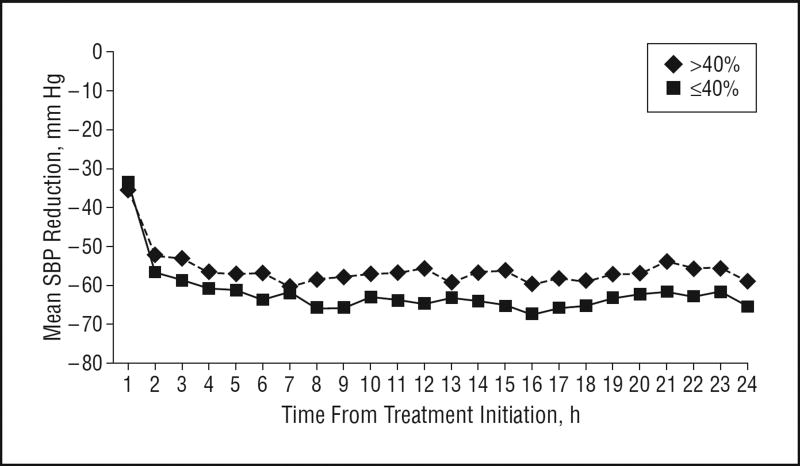
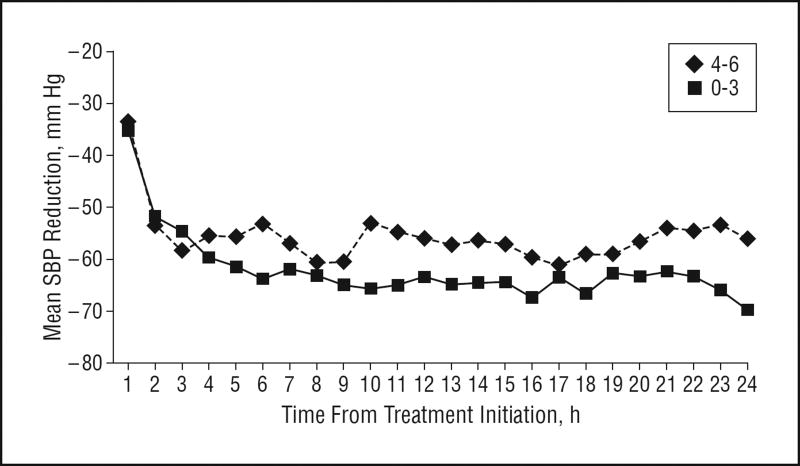
Main outcome measures: We evaluated the effect of SBP reduction (relative to initial SBP) on the following: hematoma expansion (defined as an increased intraparenchymal hemorrhage volume >33% on 24-hour vs baseline computed tomographic [CT] images), higher perihematomal edema ratio (defined as a >40% increased ratio of edema volume to hematoma volume on 24-hour vs baseline CT images), and poor 3-month outcome (defined as a modified Rankin scale score of 4-6).
Results: Sixty patients (mean [SD] age, 62.0 [15.1] years; 34 men) were recruited (18, 20, and 22 patients in each of the 3 SBP reduction goal tiers). The median area under the curve (AUC) (calculated as the area between the hourly SBP measurements over 24 hours and the baseline SBP) was 1360 (minimum, 3643; maximum, 45) U. Comparing patients having less vs more aggressive SBP reduction based on 24-hour AUC analysis, frequencies were 32% vs 17% for hematoma expansion, 61% vs 40% for higher perihematomal edema ratio, and 46% vs 38% for poor 3-month outcome (P > .05 for all). The median SBP reductions were 54 mm Hg at 6 hours and 62 mm Hg at 6 hours from treatment initiation. Comparing patients having equal to or less vs more than the median SBP reduction at 2 hours, frequencies were 21% vs 31% for hematoma expansion, 42% vs 57% for higher perihematomal edema ratio, and 35% vs 48% for poor 3-month outcome (P > .05 for all).
Conclusions: We found no significant relationship between SBP reduction and any of the outcomes measured herein; however, the Antihypertensive Treatment of Acute Cerebral Hemorrhage study was primarily a safety study and was not powered for such end points. The consistent favorable direction of these associations supports further studies with an adequately powered randomized controlled design to evaluate the efficacy of aggressive pharmacologic SBP reduction.
Figures
References
-
- Qureshi AI. Acute hypertensive response in patients with stroke: pathophysiology and management. Circulation. 2008;118(2):176–187. - PubMed
-
- Kazui S, Minematsu K, Yamamoto H, Sawada T, Yamaguchi T. Predisposing factors to enlargement of spontaneous intracerebral hematoma. Stroke. 1997;28(12):2370–2375. - PubMed
-
- Dandapani BK, Suzuki S, Kelley RE, Reyes-Iglesias Y, Duncan RC. Relation between blood pressure and outcome in intracerebral hemorrhage. Stroke. 1995;26(1):21–24. - PubMed
