

Pluripotency of human embryonic and induced pluripotent stem cells for cardiac and vascular regeneration
- PMID: 20458433
- PMCID: PMC5918288
- DOI: 10.1160/TH09-07-0507
Pluripotency of human embryonic and induced pluripotent stem cells for cardiac and vascular regeneration
Abstract
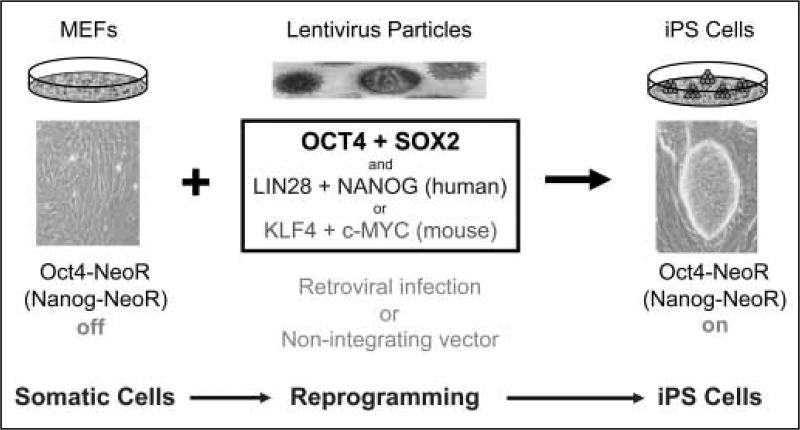
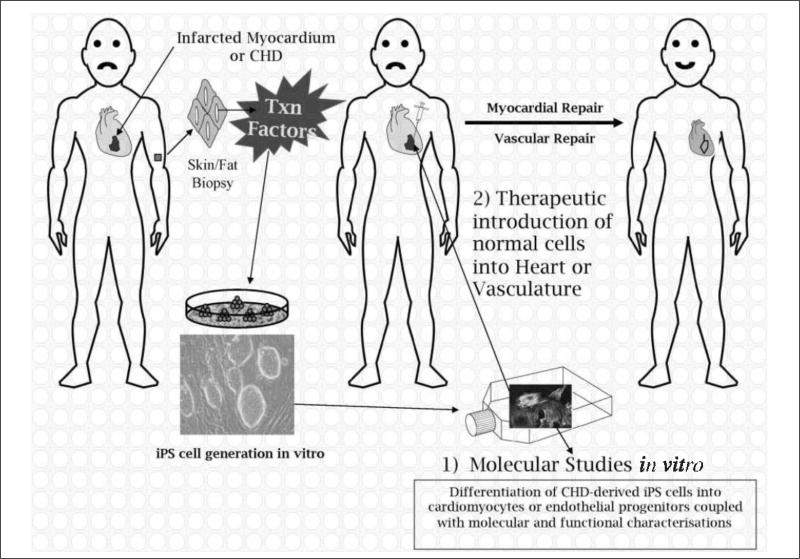
Cardiac and vascular abnormalities and disease syndromes are major causes of death both during human development and with aging. To identify the cause of congenital defects and to combat this epidemic in the aging population, new models must be created for scientific investigation and new therapies must be developed. Recent advances in pluripotent stem cell biology offer renewed hope for tackling these problems. Of particular importance has been the creation of induced pluripotent (iPS) cells from adult tissues and organs through the forced expression of two to four transcription factors. Moreover, iPS cells, which are phenotypically indistinguishable from embryonic stem (ES) cells, can be generated from any patient. This unique capacity when coupled with samples from patients who have congenital and genetic defects of unknown aetiology should permit the creation of new model systems that foment scientific investigation. Moreover, creation of patient-specific cells should overcome many of the immunological limitations that currently impede therapeutic applications associated with other pluripotent stem cells and their derivatives.The aims of this paper will be to discuss cardiac and vascular diseases and show how iPS cells may be employed to overcome some of the most significant scientific and clinical hurdles facing this field.
Figures
References
-
- Pierpont ME, Basson CT, Benson DW, et al. Genetic basis for congenital heart defects: Current knowledge – A scientific statement from the American heart association congenital cardiac defects committee, council on cardiovascular disease in the young. Circulation. 2007;115:3015–3038. - PubMed
-
- Najjar SS, Scuteri A, Lakatta EG. Arterial aging – Is it an immutable cardiovascular risk factor? Hypertension. 2005;46:454–462. - PubMed
-
- Steffens S, Montecucco F, Mach F. The inflammatory response as a target to reduce myocardial ischaemia and reperfusion injury. Thromb Haemost. 2009;102:240–247. - PubMed
