

Primary endoscopic approximation suture under cap-assisted endoscopy of an ERCP-induced duodenal perforation
- PMID: 20458771
- PMCID: PMC2868227
- DOI: 10.3748/wjg.v16.i18.2305
Primary endoscopic approximation suture under cap-assisted endoscopy of an ERCP-induced duodenal perforation
Abstract
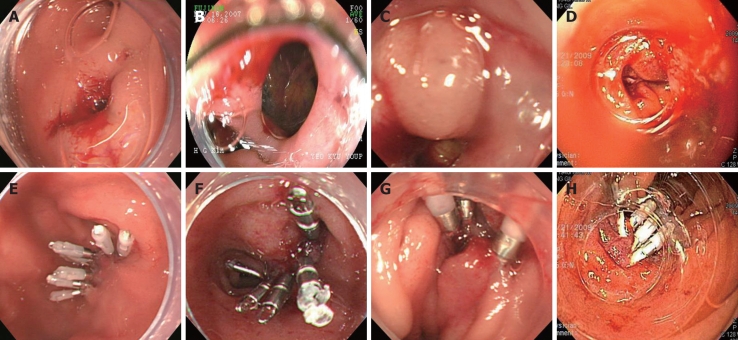
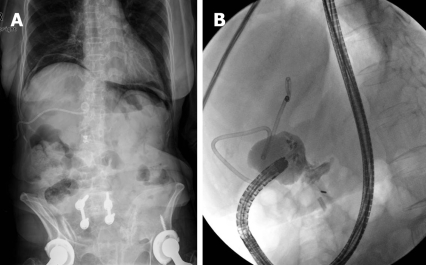
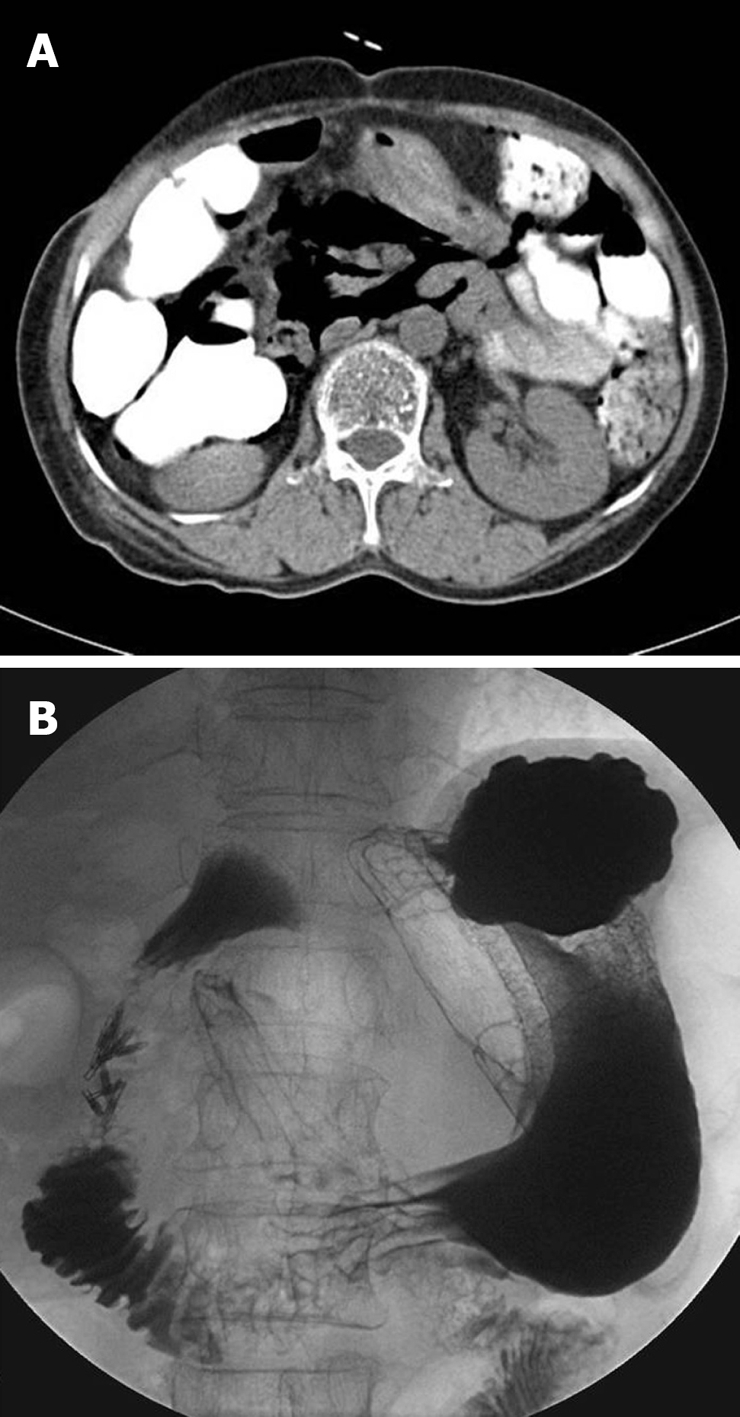
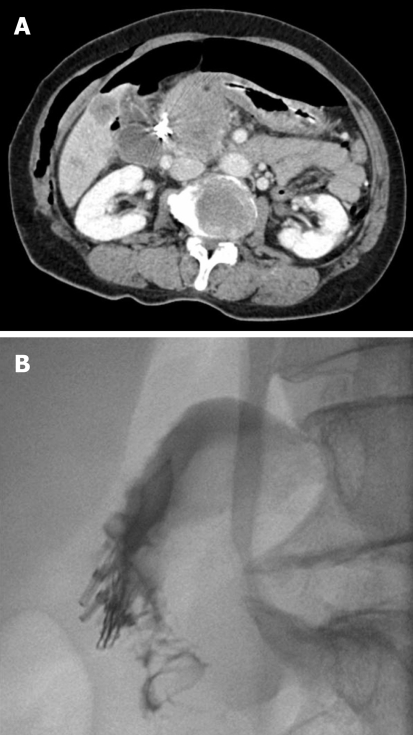
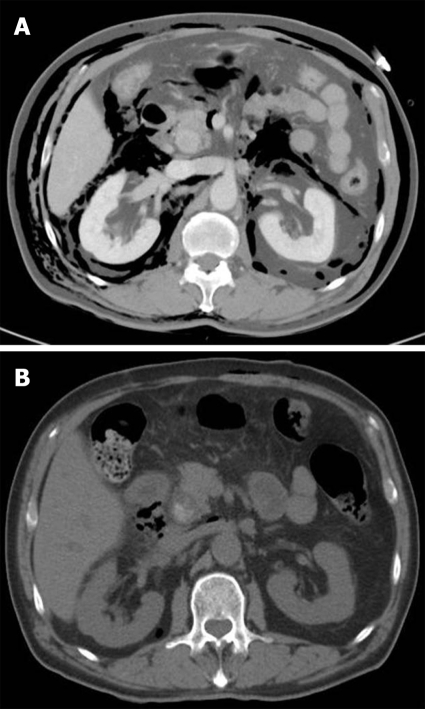
Duodenal perforation during endoscopic retrograde cholangiopancreatography (ERCP) is a rare complication, but it has a relatively high mortality risk. Early diagnosis and prompt management are key factors for the successful treatment of ERCP-related perforation. The management of perforation can initially be conservative in cases resulting from sphincterotomy or guide wire trauma. However, the current standard treatment for duodenal free wall perforation is surgical repair. Recently, several case reports of endoscopic closure techniques using endoclips, endoloops, or fully covered metal stents have been described. We describe four cases of iatrogenic duodenal bulb or lateral wall perforation caused by the scope tip that occurred during ERCP in tertiary referral centers. All the cases were simply managed by endoclips under transparent cap-assisted endoscopy. Based on the available evidence and our experience, endoscopic closure was a safe and feasible method even for duodenoscope-induced perforations. Our results suggest that endoscopists may be more willing to use this treatment.
Figures
References
-
- Fatima J, Baron TH, Topazian MD, Houghton SG, Iqbal CW, Ott BJ, Farley DR, Farnell MB, Sarr MG. Pancreaticobiliary and duodenal perforations after periampullary endoscopic procedures: diagnosis and management. Arch Surg. 2007;142:448–454; discussion 454-455. - PubMed
-
- Vandervoort J, Soetikno RM, Tham TC, Wong RC, Ferrari AP Jr, Montes H, Roston AD, Slivka A, Lichtenstein DR, Ruymann FW, et al. Risk factors for complications after performance of ERCP. Gastrointest Endosc. 2002;56:652–656. - PubMed
-
- Howard TJ, Tan T, Lehman GA, Sherman S, Madura JA, Fogel E, Swack ML, Kopecky KK. Classification and management of perforations complicating endoscopic sphincterotomy. Surgery. 1999;126:658–663; discussion 664-665. - PubMed
-
- Enns R, Eloubeidi MA, Mergener K, Jowell PS, Branch MS, Pappas TM, Baillie J. ERCP-related perforations: risk factors and management. Endoscopy. 2002;34:293–298. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
