

Radiological diagnosis of duodenocaval fistula: a case report and literature review
- PMID: 20458773
- PMCID: PMC2868229
- DOI: 10.3748/wjg.v16.i18.2314
Radiological diagnosis of duodenocaval fistula: a case report and literature review
Abstract
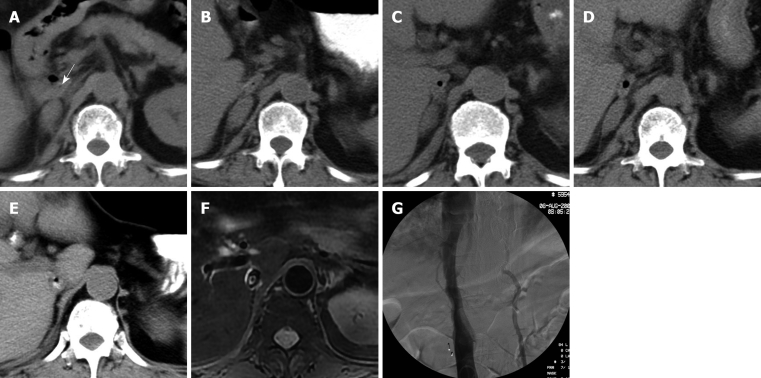
Duodenocaval fistula (DCF) is an uncommon but lethal clinical entity. The high mortality has been attributed to the difficulty of diagnosis before attempts at definitive therapy. In this case report, we describe a patient with a series of computed tomography (CT) examinations over a 2-mo period in hospital. A low-density air bubble appeared in the inferior vena cava (IVC) on the second day in hospital and became clear on day 19, and gradually enlarged. Magnetic resonance imaging (MRI) also clearly demonstrated a high-signal enteric contrast medium or thrombus and signal-void air bubbles in the IVC. However, cavography did not show the filling defect. We suggest that noninvasive CT and MRI should be chosen as a first-line investigation, and IVC, including the surrounding structures, should be carefully reviewed on images if DCF is clinically considered.
Figures
References
-
- Perera GB, Wilson SE, Barie PS, Butler JA. Duodenocaval fistula: a late complication of retroperitoneal irradiation and vena cava replacement. Ann Vasc Surg. 2004;18:52–58. - PubMed
-
- Moran EA, Porterfield JR Jr, Nagorney DM. Duodenocaval fistula after irradiation and resection of a retroperitoneal sarcoma. J Gastrointest Surg. 2008;12:776–778. - PubMed
-
- Guillem PG, Binot D, Dupuy-Cuny J, Laberenne JE, Lesage J, Triboulet JP, Chambon JP. Duodenocaval fistula: a life-threatening condition of various origins. J Vasc Surg. 2001;33:643–645. - PubMed
-
- Benjamin DS, Ruckle HC, Hadley HR. Local recurrence of renal cell carcinoma causing duodenal-inferior vena caval fistula: case report and review of the literature. Urology. 1996;48:636–638. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
