

Incremental value of contrast myocardial perfusion to detect intermediate versus severe coronary artery stenosis during stress-echocardiography
- PMID: 20459632
- PMCID: PMC2877655
- DOI: 10.1186/1476-7120-8-16
Incremental value of contrast myocardial perfusion to detect intermediate versus severe coronary artery stenosis during stress-echocardiography
Abstract
Background: We aimed to compare the incremental value of contrast myocardial perfusion imaging (MPI) for the detection of intermediate versus severe coronary artery stenosis during dipyridamole-atropine echocardiography (DASE).Wall motion (WM) assessment during stress-echocardiography demonstrates suboptimal sensitivity to detect coronary artery disease (CAD), particularly in patients with isolated intermediate (50%-70%) coronary stenosis.
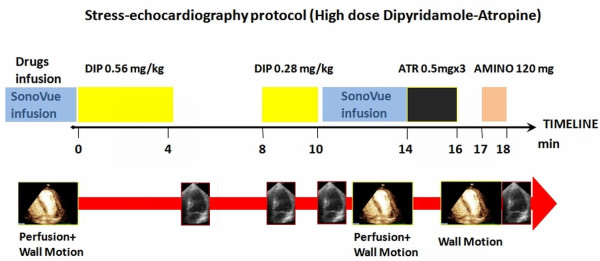
Methods: We performed DASE with MPI in 150 patients with a suspected chest pain syndrome who were given clinical indication to coronary angiography.
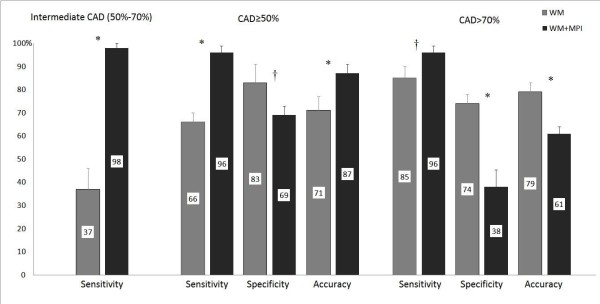
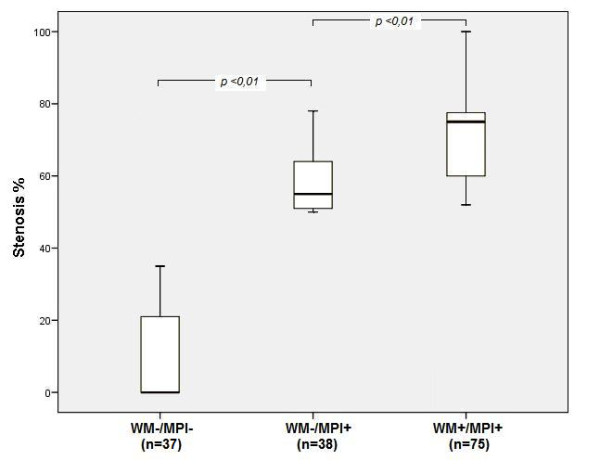
Results and discussion: When CAD was defined as the presence of a >or=50% stenosis, the addition of MPI increased sensitivity (+30%) and decreased specificity (-14%), with a final increase in total diagnostic accuracy (+16%, p < 0.001). The addition of MPI data substantially increased the sensitivity to detect patients with isolated intermediate stenosis from 37% to 98% (p < 0.001); the incremental sensitivity was much lower in patients with severe stenosis, from 85% to 96% (p < 0.05), at the expense of a higher decrease in specificity and a final decrease in total diagnostic accuracy (-18%, p < 0.001).
Conclusions: The addition of MPI on top of WM analysis during DASE increases the diagnostic sensitivity to detect obstructive CAD, whatever its definition (>or=50% or > 70% stenosis), but it is mainly driven by the sensitivity increase in the intermediate group (50%-70% stenosis).The total diagnostic accuracy increased only when defining CAD as >or=50% stenosis, since in patients with severe stenosis (> 70%) the decrease in specificity is not counterbalanced by the minor sensitivity increase.
Figures

Similar articles
-
Detection of coronary artery disease by combined assessment of wall motion, myocardial perfusion and coronary flow reserve: a multiparametric contrast stress-echocardiography study.J Am Soc Echocardiogr. 2010 Dec;23(12):1242-50. doi: 10.1016/j.echo.2010.09.003. Epub 2010 Oct 15. J Am Soc Echocardiogr. 2010. PMID: 20951000
-
Contrast stress echocardiography for the diagnosis of coronary artery disease in patients with chest pain but without acute coronary syndrome: incremental value of myocardial perfusion.J Am Soc Echocardiogr. 2009 Apr;22(4):404-10. doi: 10.1016/j.echo.2009.01.017. J Am Soc Echocardiogr. 2009. PMID: 19345309 Clinical Trial.
-
Detection of significant coronary artery disease by noninvasive anatomical and functional imaging.Circ Cardiovasc Imaging. 2015 Mar;8(3):e002179. doi: 10.1161/CIRCIMAGING.114.002179. Circ Cardiovasc Imaging. 2015. PMID: 25711274 Clinical Trial.
-
The diagnostic accuracy of pharmacological stress echocardiography for the assessment of coronary artery disease: a meta-analysis.Cardiovasc Ultrasound. 2008 Jun 19;6:30. doi: 10.1186/1476-7120-6-30. Cardiovasc Ultrasound. 2008. PMID: 18565214 Free PMC article. Review.
-
Diagnostic accuracy of myocardial perfusion imaging and stress echocardiography for the diagnosis of left main and triple vessel coronary artery disease: a comparative meta-analysis.Heart. 2010 Jun;96(12):956-66. doi: 10.1136/hrt.2009.182295. Heart. 2010. PMID: 20538671 Review.
Cited by
-
Contrast echocardiography for detection of myocardial perfusion abnormalities : A clinical perspective.Herz. 2017 May;42(3):287-294. doi: 10.1007/s00059-017-4536-7. Herz. 2017. PMID: 28188323 Review. English.
-
Evolution of Stress Echocardiogram in the Era of CT Angiography.Cureus. 2023 May 25;15(5):e39501. doi: 10.7759/cureus.39501. eCollection 2023 May. Cureus. 2023. PMID: 37378169 Free PMC article. Review.
-
Stress Echocardiography: Need to Optimize its Appropriate Use in Suspected Angina and a Review of Available Additional Tools for its Clinical Application in 2018: First do no Harm! Second do it at the Highest Possible Accuracy.J Cardiovasc Echogr. 2018 Jul-Sep;28(3):154-159. doi: 10.4103/jcecho.jcecho_16_18. J Cardiovasc Echogr. 2018. PMID: 30306018 Free PMC article. Review.
-
Two methods for increasing sensitivity of dobutamine stress echocardiography: strain imaging and heart-type fatty acid-binding protein levels.Anatol J Cardiol. 2016 Mar;16(3):210-1. doi: 10.14744/AnatolJCardiol.2016.6704. Anatol J Cardiol. 2016. PMID: 27067556 Free PMC article. No abstract available.
-
The Role of Non-Invasive Multimodality Imaging in Chronic Coronary Syndrome: Anatomical and Functional Pathways.Diagnostics (Basel). 2023 Jun 16;13(12):2083. doi: 10.3390/diagnostics13122083. Diagnostics (Basel). 2023. PMID: 37370978 Free PMC article. Review.
References
-
- Elhendy A, O'Leary EL, Xie F, McGrain AC, Anderson JR, Porter TR. Comparative accuracy of real-time myocardial contrast perfusion imaging and wall motion analysis during dobutamine stress echocardiography for the diagnosis of coronary artery disease. J Am Coll Cardiol. 2004;44:2185–91. doi: 10.1016/j.jacc.2004.08.059. - DOI - PubMed
-
- Rigo F, Sicari R, Gherardi S, Djordjevic-Dikic A, Cortigiani L, Picano E. Prognostic value of coronary flow reserve in medically treated patients with left anterior descending coronary disease with stenosis 51% to 75% in diameter. Am J Cardiol. 2007;100:1527–31. doi: 10.1016/j.amjcard.2007.06.060. - DOI - PubMed
-
- Nagel E, Lehmkuhl HB, Bocksch W, Klein C, Vogel U, Frantz E, Ellmer A, Dreysse S, Fleck E. Noninvasive diagnosis of ischemia-induced wall motion abnormalities with the use of high-dose dobutamine stress MRI: comparison with dobutamine stress echocardiography. Circulation. 1999;99:763–70. - PubMed
-
- Berger A, Botman KJ, MacCarthy PA, Wijns W, Bartunek J, Heyndrickx GR, Pijls NH, De Bruyne B. Long-term clinical outcome after fractional flow reserve-guided percutaneous coronary intervention in patients with multivessel disease. J Am Coll Cardiol. 2005;46:438–42. doi: 10.1016/j.jacc.2005.04.041. - DOI - PubMed
-
- Wei K, Ragosta M, Thorpe J, Coggins M, Moos S, Kaul S. Noninvasive quantification of coronary blood flow reserve in humans using myocardial contrast echocardiography. Circulation. 2001;103:2560–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
