

Towards a more efficient diabetes control in primary care: six-monthly monitoring compared with three-monthly monitoring in type 2 diabetes - The EFFIMODI trial. Design of a randomised controlled patient-preference equivalence trial in primary care
- PMID: 20459820
- PMCID: PMC2885321
- DOI: 10.1186/1471-2296-11-35
Towards a more efficient diabetes control in primary care: six-monthly monitoring compared with three-monthly monitoring in type 2 diabetes - The EFFIMODI trial. Design of a randomised controlled patient-preference equivalence trial in primary care
Abstract
Background: Scientific evidence for the frequency of monitoring of type 2 diabetes patients is lacking. If three-monthly control in general practice could be reduced to six-monthly control in some patients, this would on the one hand reduce the use of medical services including involvement of practice nurses, and thus reduce costs, and on the other hand alleviate the burden of people with type 2 diabetes. The goal of this study is to make primary diabetes care as efficient as possible for patients and health care providers. Therefore, we want to determine whether six-monthly monitoring of well-controlled type 2 diabetes patients in primary care leads to equivalent cardiometabolic control compared to the generally recommended three-monthly monitoring.
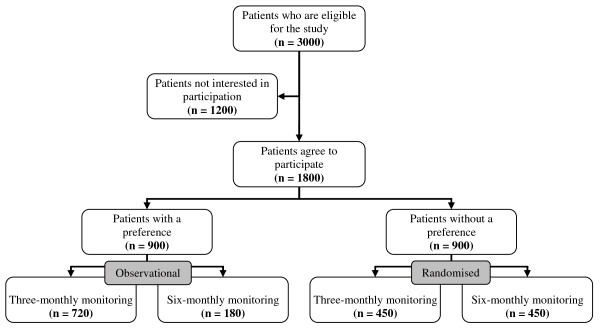
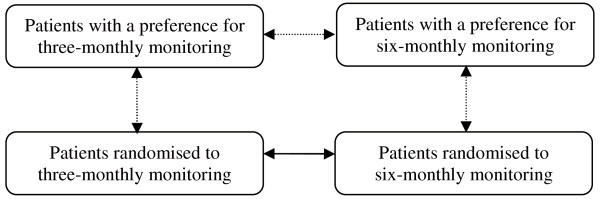
Methods and design: The study is a randomised controlled patient-preference equivalence trial. Participants are asked if they prefer three-monthly (usual care) or six-monthly diabetes monitoring. If they do not have a preference, they are randomised to a three-monthly or six-monthly monitoring group. Patients are eligible for the study if they are between 40 and 80 years old, diagnosed with type 2 diabetes more than one year ago, treated by a general practitioner, not on insulin treatment, and with HbA1c < or = 7.5%, systolic blood pressure < or = 145 mmHg and total cholesterol < or = 5.2 mmol/l. The intervention group (six-monthly monitoring) will receive the same treatment with the same treatment targets as the control group (three-monthly monitoring). The intervention period will last one and a half year. After the intervention, the three-monthly and six-monthly monitoring groups are compared on equivalence of cardiometabolic control. Secondary outcome measures are HbA1c, blood pressure, cholesterol level, Body Mass Index, smoking behaviour, physical activity, loss of work due to illness, health status, diabetes-specific distress, satisfaction with treatment and adherence to medications. We will use intention-to-treat analysis with repeated measures. For outcomes that have only baseline and final measurements, we will use ANCOVA. Depending on the results, a cost-minimisation analysis or an incremental cost-effectiveness analysis will be done.
Discussion: This study will provide valuable information on the most efficient control frequency of well-controlled type 2 diabetes patients in primary care.
Figures
Similar articles
-
Satisfaction of well-controlled type 2 diabetes patients with three-monthly and six-monthly monitoring.BMC Fam Pract. 2013 Jul 30;14:107. doi: 10.1186/1471-2296-14-107. BMC Fam Pract. 2013. PMID: 23899039 Free PMC article. Clinical Trial.
-
Effectiveness and cost-effectiveness of 3-monthly versus 6-monthly monitoring of well-controlled type 2 diabetes patients: a pragmatic randomised controlled patient-preference equivalence trial in primary care (EFFIMODI study).Diabetes Obes Metab. 2014 Sep;16(9):841-9. doi: 10.1111/dom.12288. Epub 2014 Apr 9. Diabetes Obes Metab. 2014. PMID: 24635880 Clinical Trial.
-
Six-monthly diabetes monitoring of well-controlled patients: experiences of primary care providers.Prim Care Diabetes. 2013 Oct;7(3):187-91. doi: 10.1016/j.pcd.2013.04.005. Epub 2013 May 7. Prim Care Diabetes. 2013. PMID: 23660331 Clinical Trial.
-
Psychological interventions to improve self-management of type 1 and type 2 diabetes: a systematic review.Health Technol Assess. 2020 Jun;24(28):1-232. doi: 10.3310/hta24280. Health Technol Assess. 2020. PMID: 32568666 Free PMC article.
-
Meta-analysis of individual patient data in randomised trials of self monitoring of blood glucose in people with non-insulin treated type 2 diabetes.BMJ. 2012 Feb 27;344:e486. doi: 10.1136/bmj.e486. BMJ. 2012. PMID: 22371867
Cited by
-
Health-related quality of life (HRQoL) from HIV patients' perspective: comparison of patient-reported outcome (PRO) measures among people living with hiv (PLWH) and other chronic clinical conditions.J Patient Rep Outcomes. 2022 Mar 26;6(1):27. doi: 10.1186/s41687-022-00423-4. J Patient Rep Outcomes. 2022. PMID: 35347476 Free PMC article.
-
Effectiveness of monthly and bimonthly follow-up of patients with well-controlled type 2 diabetes: a propensity score matched cohort study.BMC Endocr Disord. 2019 May 2;19(1):43. doi: 10.1186/s12902-019-0372-5. BMC Endocr Disord. 2019. PMID: 31046742 Free PMC article.
-
Satisfaction of well-controlled type 2 diabetes patients with three-monthly and six-monthly monitoring.BMC Fam Pract. 2013 Jul 30;14:107. doi: 10.1186/1471-2296-14-107. BMC Fam Pract. 2013. PMID: 23899039 Free PMC article. Clinical Trial.
-
Both cardiovascular and non-cardiovascular comorbidity are related to health status in well-controlled type 2 diabetes patients: a cross-sectional analysis.Cardiovasc Diabetol. 2012 Oct 5;11:121. doi: 10.1186/1475-2840-11-121. Cardiovasc Diabetol. 2012. PMID: 23039172 Free PMC article.
References
-
- Baan CA, Poos MJJC. Volksgezondheid Toekomst Verkenning, Nationaal Kompas Volksgezondheid. Bilthoven, RIVM; 2009. Hoe vaak komt diabetes mellitus voor en hoeveel mensen sterven eraan? [in Dutch]
-
- van den Berg MJ, Kolthof ED, de Bakker DH, Zee J van der. Tweede Nationale Studie naar ziekten en verrichtingen in de huisartspraktijk: de werkbelasting van huisartsen [in Dutch] Utrecht: NIVEL; 2004.
-
- Rutten GEHM, De Grauw WJC, Nijpels G, Goudswaard AN, Uitewaal PJM, van der Does FEE. NHG-standaard Diabetes mellitus type 2 [article in Dutch] Huisarts Wet. 2006;49:137–152.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
