

Beneficial effects of loxapine on agitation and breathing patterns during weaning from mechanical ventilation
- PMID: 20459867
- PMCID: PMC2911718
- DOI: 10.1186/cc9015
Beneficial effects of loxapine on agitation and breathing patterns during weaning from mechanical ventilation
Abstract
Introduction: Interruption of sedation during weaning from mechanical ventilation often leads to patient agitation because of withdrawal syndrome. We tested the short-term efficacy and tolerance of loxapine in this situation.
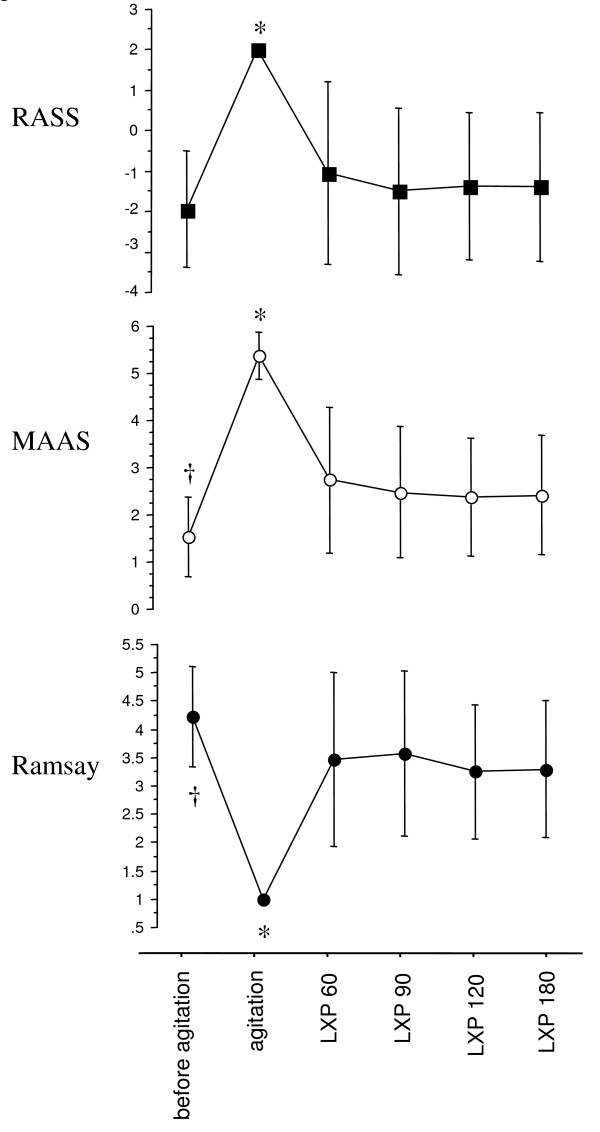
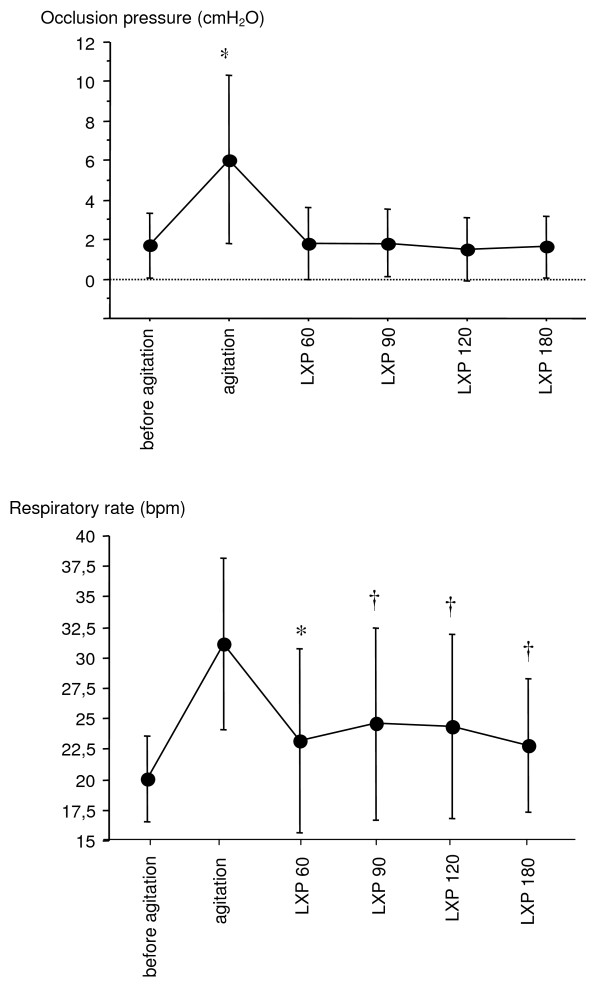
Methods: Nineteen mechanically ventilated patients with marked agitation after sedation withdrawal were included. Three agitation scales, the Richmond Agitation Sedation Scale (RASS), the Motor Activity Assessment Scale (MAAS), and the Ramsay and physiological variables (respiratory rate, airway occlusion pressure during the first 0.1 second of inspiration (P0.1), heart rate and systolic arterial blood pressure) were recorded before and after loxapine administration.
Results: Loxapine dramatically improved all agitation scores (RASS and MASS decreased from 2 +/- 0 to -1.1 +/- 2.3, and 5.4 +/- 0.5 to 2.7 +/- 1.6, respectively; Ramsay increased from 1.0 +/- 0 to 3.5 +/- 1.5, 60 minutes after loxapine administration, P < 0.05 for all scores) as well as P0.1 (6 +/- 4.2 to 1.8 +/- 1.8 cm H2O; P < 0.05) and respiratory rate (from 31.2 +/- 7.2 to 23.4 +/- 7.8; P < 0.05) without hemodynamic adverse events. No side effects occurred. Sixteen (84%) patients were successfully managed with loxapine, sedation was resumed in two others, and one patient self-extubated without having to be reintubated.
Conclusions: Loxapine was safe and effective in treating agitation in a small group of mechanically ventilated patients and improved respiratory physiologic parameters, enabling the weaning process to be pursued. A multicenter trial is under way to confirm these promising results.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
