

The impact of removing financial incentives from clinical quality indicators: longitudinal analysis of four Kaiser Permanente indicators
- PMID: 20460330
- PMCID: PMC2868163
- DOI: 10.1136/bmj.c1898
The impact of removing financial incentives from clinical quality indicators: longitudinal analysis of four Kaiser Permanente indicators
Abstract
Objective: To evaluate the effect of financial incentives on four clinical quality indicators common to pay for performance plans in the United Kingdom and at Kaiser Permanente in California.
Design: Longitudinal analysis.
Setting: 35 medical facilities of Kaiser Permanente Northern California, 1997-2007.
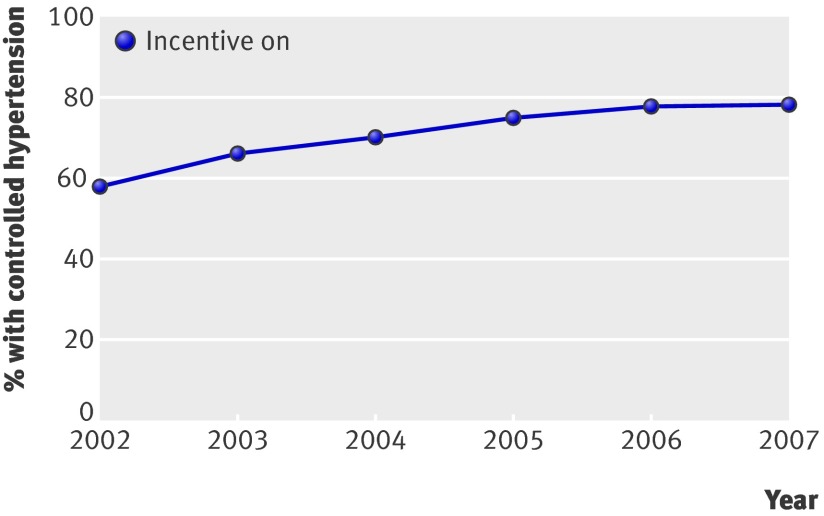
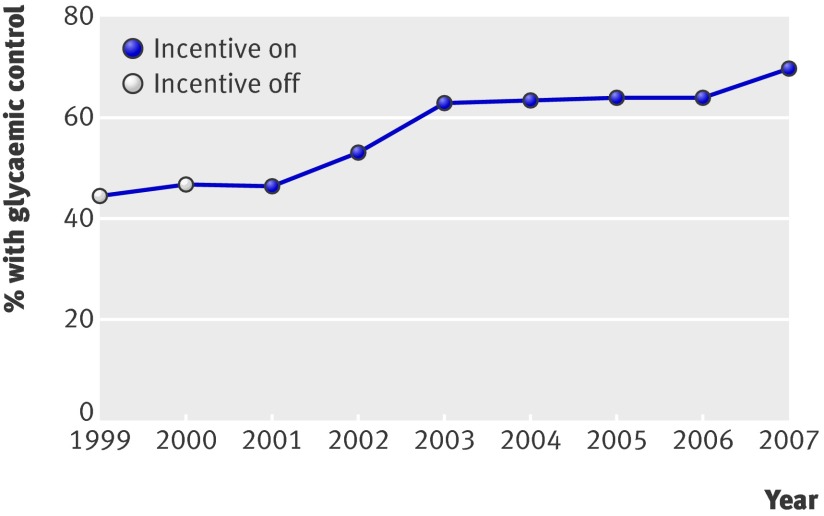
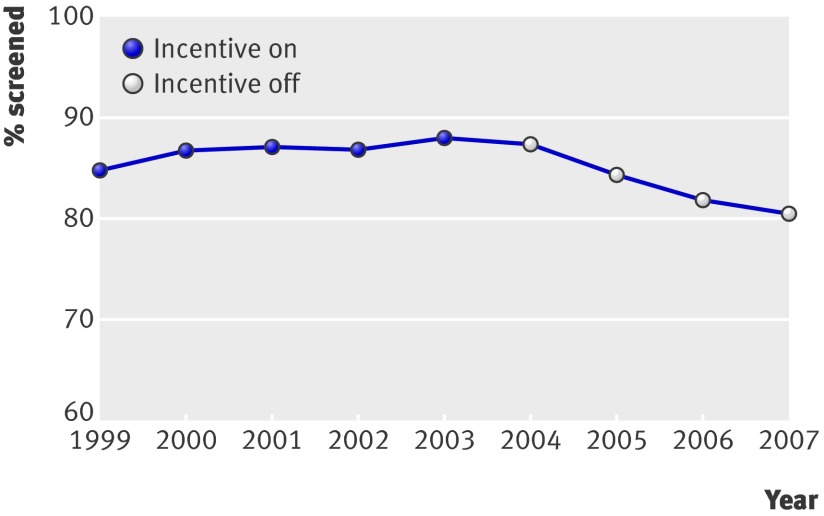
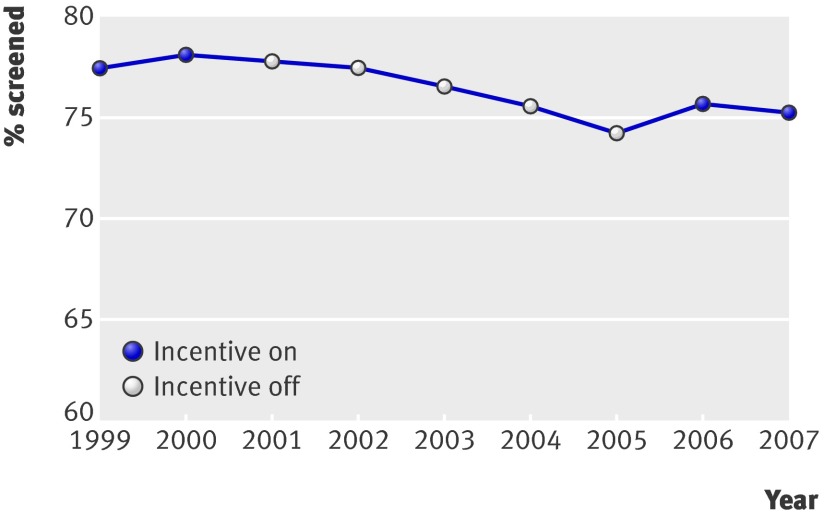
Participants: 2 523 659 adult members of Kaiser Permanente Northern California. Main outcomes measures Yearly assessment of patient level glycaemic control (HbA(1c) <8%), screening for diabetic retinopathy, control of hypertension (systolic blood pressure <140 mm Hg), and screening for cervical cancer.
Results: Incentives for two indicators-screening for diabetic retinopathy and for cervical cancer-were removed during the study period. During the five consecutive years when financial incentives were attached to screening for diabetic retinopathy (1999-2003), the rate rose from 84.9% to 88.1%. This was followed by four years without incentives when the rate fell year on year to 80.5%. During the two initial years when financial incentives were attached to cervical cancer screening (1999-2000), the screening rate rose slightly, from 77.4% to 78.0%. During the next five years when financial incentives were removed, screening rates fell year on year to 74.3%. Incentives were then reattached for two years (2006-7) and screening rates began to increase. Across the 35 facilities, the removal of incentives was associated with a decrease in performance of about 3% per year on average for screening for diabetic retinopathy and about 1.6% per year for cervical cancer screening.
Conclusion: Policy makers and clinicians should be aware that removing facility directed financial incentives from clinical indicators may mean that performance levels decline.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
References
-
- Lindenauer PK, Remus D, Roman S, Rothberg MB, Benjamin EM, Ma A, et al. Public reporting and pay for performance in hospital quality improvement. N Engl J Med 2007;356:486-96. - PubMed
-
- Rosenthal MB, Frank RG, Li Z, Epstein AM. Early experience with pay for performance: from concept to practice. JAMA 2005;294:1788-93. - PubMed
-
- Campbell SM, Reeves D, Kontopantelis E, Middleton E, Sibbald B, Roland M. Quality of primary care in England with the introduction of pay for performance. N Engl J Med 2007;357:181-90. - PubMed
-
- Ganz D, Wenger NS, Roth C, Kamberg CJ, Chang JT, MacLean CH, et al. The effect of a quality improvement initiative on the quality of other aspects of health care: the law of unintended consequences? Med Care 2007;45:8-18. - PubMed
-
- Ryan RM, Deci EL. Self determination theory and the facilitation of intrinsic motivation, social development and well-being. Am Psychol 2000;55:68-78. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous