

Simvastatin as a treatment for pulmonary hypertension trial
- PMID: 20460548
- PMCID: PMC2874452
- DOI: 10.1164/rccm.2009111-699oc
Simvastatin as a treatment for pulmonary hypertension trial
Abstract
Rationale: In animal models of pulmonary hypertension, simvastatin has been shown to reduce pulmonary artery pressure and induce regression of associated right ventricular (RV) hypertrophy.
Objectives: To assess the therapeutic value of simvastatin in patients with pulmonary arterial hypertension (PAH).
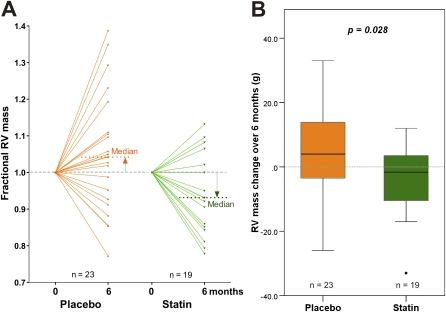
Methods: Forty-two patients with PAH were randomized to receive either simvastatin (80 mg/d) or placebo in addition to current care for 6 months, and thereafter offered open-label simvastatin. The primary outcome was change in RV mass, assessed by cardiac magnetic resonance (CMR).
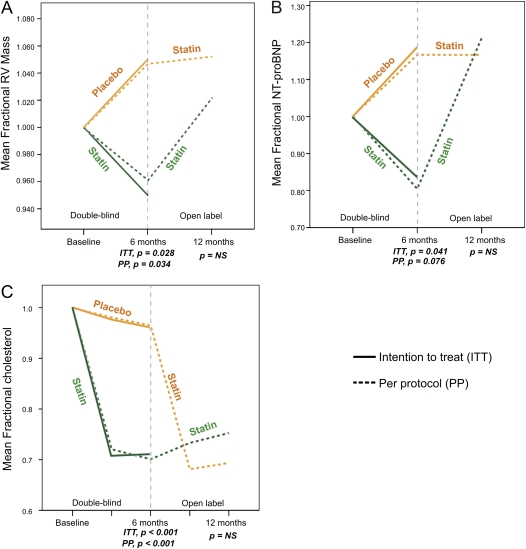
Measurements and main results: At 6 months, RV mass decreased by 5.2 +/- 11 g in the statin group (P = 0.045) and increased 3.9 +/- 14 g in the placebo group. The treatment effect was -9.1 g (P = 0.028). N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels decreased significantly in the statin group (-75 +/- 167 fmol/ml; P = 0.02) but not the placebo group (49 +/- 224 fmol/ml; P = 0.43; overall treatment effect -124 fmol/ml; P = 0.041). There were no significant changes in other outcome measures (including 6-minute walk test, cardiac index, and circulating cytokines). From 6 to 12 months, both RV mass and NT-proBNP increased toward baseline values in 16 patients on active treatment who continued with simvastatin but remained stable in 18 patients who switched from placebo to simvastatin. Two patients required a reduction in dose but not cessation of simvastatin.
Conclusions: Simvastatin added to conventional therapy produces a small and transient early reduction in RV mass and NT-proBNP levels in patients with PAH, but this is not sustained over 12 months.
Trial registration: ClinicalTrials.gov NCT00180713.
Figures


References
-
- Hassoun PM, Mouthon L, Barbera JA, Eddahibi S, Flores SC, Grimminger F, Jones PL, Maitland ML, Michelakis ED, Morrell NW, et al. Inflammation, growth factors, and pulmonary vascular remodeling. J Am Coll Cardiol 2009;54:S10–S19. - PubMed
-
- NationalPulmonary Hypertension Centres of the UK and Ireland. Consensus statement on the management of pulmonary hypertension in clinical practice in the UK and Ireland. Thorax 2008;63:ii1–ii41. - PubMed
-
- Girgis RE, Li D, Zhan X, Garcia JG, Tuder RM, Hassoun PM, Johns RA. Attenuation of chronic hypoxic pulmonary hypertension by simvastatin. Am J Physiol Heart Circ Physiol 2003;285:H938–H945. - PubMed
-
- Guerard P, Rakotoniaina Z, Goirand F, Rochette L, Dumas M, Lirussi F, Bardou M. The HMG-CoA reductase inhibitor, pravastatin, prevents the development of monocrotaline-induced pulmonary hypertension in the rat through reduction of endothelial cell apoptosis and overexpression of eNOS. Naunyn Schmiedebergs Arch Pharmacol 2006;373:401–414. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
