

Evaluation of left atrial volumes using multidetector computed tomography: comparison with echocardiography
- PMID: 20461182
- PMCID: PMC2864855
- DOI: 10.3348/kjr.2010.11.3.286
Evaluation of left atrial volumes using multidetector computed tomography: comparison with echocardiography
Abstract
Objective: To prospectively assess the relationship between the two different measurement methods for the evaluation of left atrial (LA) volume using cardiac multidetector computed tomography (MDCT) and to compare the results between cardiac MDCT and echocardiography.
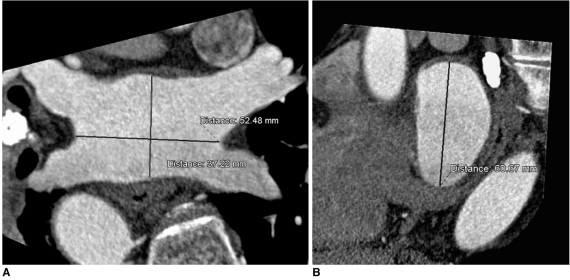
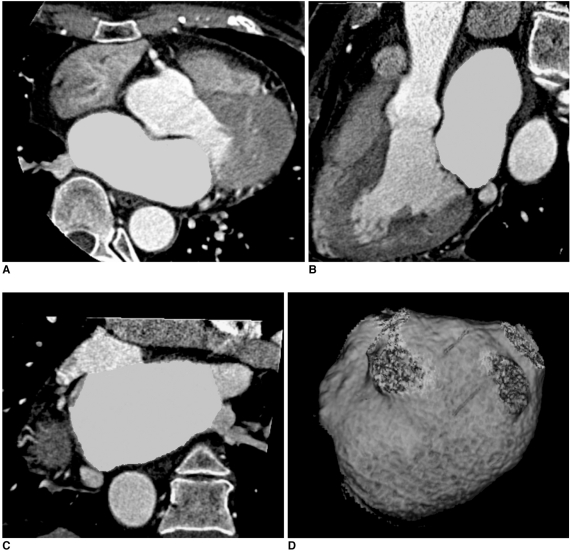
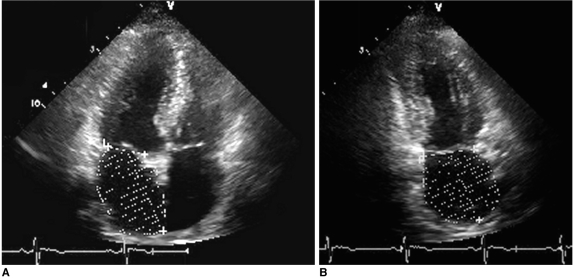
Materials and methods: Thirty-five patients (20 men, 15 women; mean age, 60 years) underwent cardiac MDCT angiography for coronary artery disease. The LA volumes were measured using two different methods: the two dimensional (2D) length-based (LB) method measured along the three-orthogonal planes of the LA and the 3D volumetric threshold-based (VTB) method measured according to the threshold 3D segmentation of the LA. The results obtained by cardiac MDCT were compared with those obtained by echocardiography.
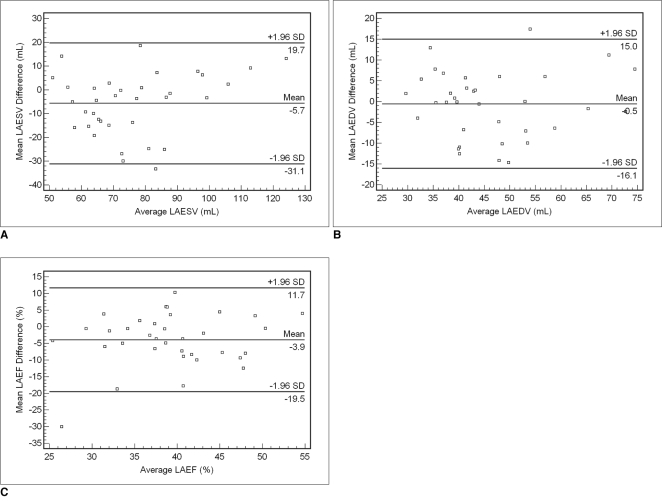
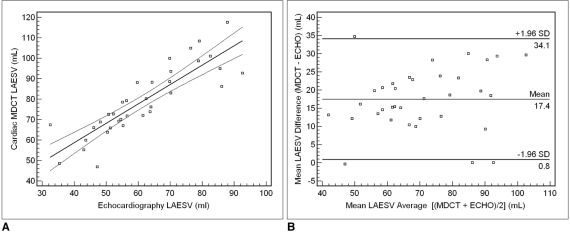
Results: The LA end-systolic and end-diastolic volumes (LAESV and LAEDV) measured by the 2D-LB method correlated well with those measured by the 3D-VTB method using cardiac MDCT (r = 0.763, r = 0.786, p = 0.001). However, there was a significant difference in the LAESVs between the two measurement methods using cardiac MDCT (p < 0.05). The LAESV measured by cardiac MDCT correlated well with measurements by echocardiography (r = 0.864, p = 0.001), however with a significant difference (p < 0.01) in their volumes. The cardiac MDCT overestimated the LAESV by 22% compared to measurements by echocardiography.
Conclusion: A significant correlation was found between the two different measurement methods for evaluating LA volumes by cardiac MDCT. Further, cardiac MDCT correlates well with echocardiography in evaluating the LA volume. However, there are significant differences in the LAESV between the two measurement methods using cardiac MDCT and between cardiac MDCT and echocardiography.
Keywords: 2D and 3D measurements; Echocardiography; Left atrial volume; Multidetector computed tomography; Simpson method.
Figures
Similar articles
-
Quantitative assessment of left atrial volume by electrocardiographic-gated contrast-enhanced multidetector computed tomography.J Cardiovasc Comput Tomogr. 2009 Mar-Apr;3(2):80-7. doi: 10.1016/j.jcct.2009.02.002. Epub 2009 Feb 14. J Cardiovasc Comput Tomogr. 2009. PMID: 19332340 Free PMC article.
-
Cardiac chamber volumes, function, and mass as determined by 64-multidetector row computed tomography: mean values among healthy adults free of hypertension and obesity.JACC Cardiovasc Imaging. 2008 Nov;1(6):782-6. doi: 10.1016/j.jcmg.2008.04.015. JACC Cardiovasc Imaging. 2008. PMID: 19356515
-
Sex-specific biatrial volumetric measurements obtained with use of multidetector computed tomography in subjects with and without coronary artery disease.Tex Heart Inst J. 2014 Jun 1;41(3):286-92. doi: 10.14503/THIJ-12-3061. eCollection 2014 Jun. Tex Heart Inst J. 2014. PMID: 24955043 Free PMC article.
-
Assessment of cardiac function using multidetector row computed tomography.J Comput Assist Tomogr. 2006 Jul-Aug;30(4):555-63. doi: 10.1097/00004728-200607000-00001. J Comput Assist Tomogr. 2006. PMID: 16845283 Review.
-
European Association of Cardiovascular Imaging/Cardiovascular Imaging Department of the Brazilian Society of Cardiology recommendations for the use of cardiac imaging to assess and follow patients after heart transplantation.Eur Heart J Cardiovasc Imaging. 2015 Sep;16(9):919-48. doi: 10.1093/ehjci/jev139. Epub 2015 Jul 2. Eur Heart J Cardiovasc Imaging. 2015. PMID: 26139361 Review.
Cited by
-
Combined Atrial Volume is Associated with Significant Atrial Arrhythmias in Total Cavopulmonary Connection Fontan Patients.Pediatr Cardiol. 2023 Dec;44(8):1741-1745. doi: 10.1007/s00246-023-03271-1. Epub 2023 Aug 24. Pediatr Cardiol. 2023. PMID: 37620579 Review.
-
Computed Tomography Confirms Increased Left Atrial Volume in Patients with Bayés Syndrome Referred for Catheter Ablation of Atrial Fibrillation.Diagnostics (Basel). 2024 Oct 30;14(21):2416. doi: 10.3390/diagnostics14212416. Diagnostics (Basel). 2024. PMID: 39518382 Free PMC article.
-
Association of left atrial structure and function and incident cardiovascular disease in patients with diabetes mellitus: results from multi-ethnic study of atherosclerosis (MESA).Eur Heart J Cardiovasc Imaging. 2017 Oct 1;18(10):1138-1144. doi: 10.1093/ehjci/jew332. Eur Heart J Cardiovasc Imaging. 2017. PMID: 28329137 Free PMC article.
-
Automatic quantification of left atrium volume for cardiac rhythm analysis leveraging 3D residual UNet for time-varying segmentation of ECG-gated CT.Comput Struct Biotechnol J. 2025 May 13;28:175-189. doi: 10.1016/j.csbj.2025.04.039. eCollection 2025. Comput Struct Biotechnol J. 2025. PMID: 40487246 Free PMC article.
-
Accuracy of Non-Electrocardiographically Gated Thoracic CT Angiography for Right Atrial and Right Ventricular Enlargement.Radiol Cardiothorac Imaging. 2019 Oct 31;1(4):e190008. doi: 10.1148/ryct.2019190008. eCollection 2019 Oct. Radiol Cardiothorac Imaging. 2019. PMID: 33778516 Free PMC article.
References
-
- Beinart R, Boyko V, Schwammenthal E, Kuperstein R, Sagie A, Hod H, et al. Long-term prognostic significance of left atrial volume in acute myocardial infarction. J Am Coll Cardiol. 2004;44:327–334. - PubMed
-
- Kizer JR, Bella JN, Palmieri V, Liu JE, Best LG, Lee ET, et al. Left atrial diameter as an independent predictor of first clinical cardiovascular events in middle-aged and elderly adults: the Strong Heart Study (SHS) Am Heart J. 2006;151:412–418. - PubMed
-
- Rossi A, Cicoira M, Zanolla L, Sandrini R, Golia G, Zardini P, et al. Determinants and prognostic value of left atrial volume in patients with dilated cardiomyopathy. J Am Coll Cardiol. 2002;40:1425. - PubMed
-
- Tsang TS, Barnes ME, Bailey KR, Leibson CL, Montgomery SC, Takemoto Y, et al. Left atrial volume: important risk marker of incident atrial fibrillation in 1655 older men and women. Mayo Clin Proc. 2001;76:467–475. - PubMed
-
- Feinberg MS, Waggoner AD, Kater KM, Cox JL, Lindsay BD, Perez JE. Restoration of atrial function after the maze procedure for patients with atrial fibrillation. Assessment by Doppler echocardiography. Circulation. 1994;90:II285–II292. - PubMed
