

Unicompartmental knee resurfacing: enlarged tibio-femoral contact area and reduced contact stress using novel patient-derived geometries
- PMID: 20461223
- PMCID: PMC2866246
- DOI: 10.2174/1874120701004010085
Unicompartmental knee resurfacing: enlarged tibio-femoral contact area and reduced contact stress using novel patient-derived geometries
Abstract
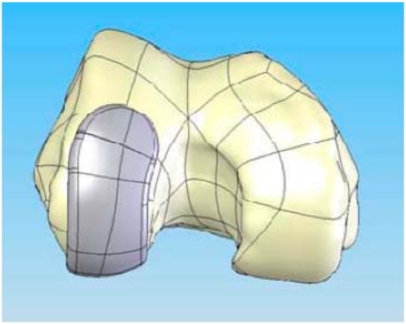
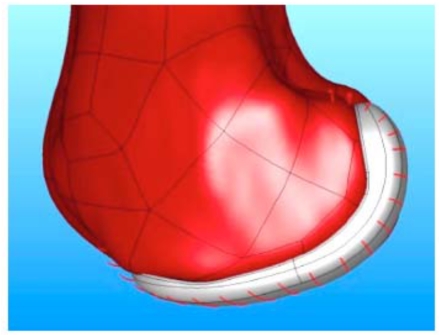
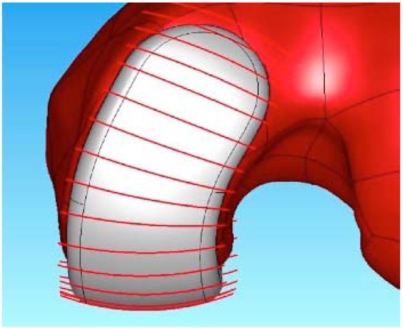
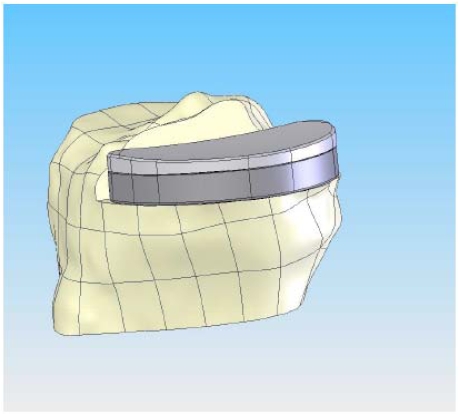
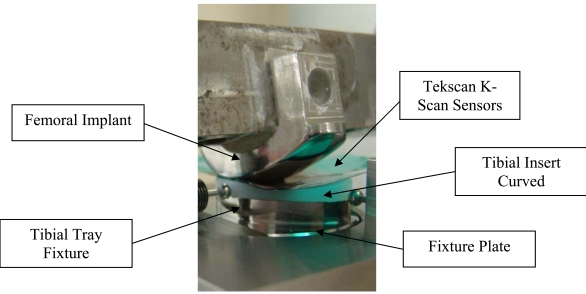
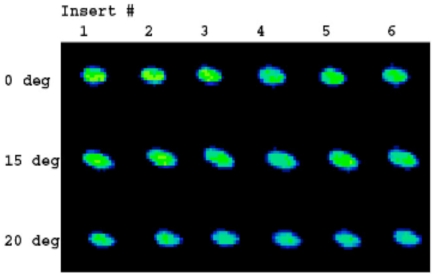
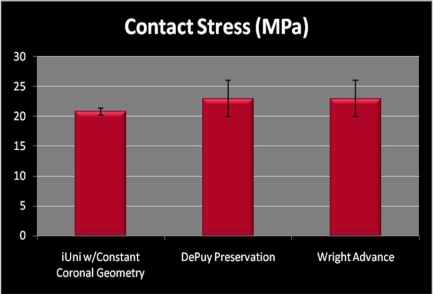
Advances in imaging technology and computer-assisted design (CAD) have recently enabled the introduction of patient-specific knee implant designs that hold the potential to improve functional performance on the basis of patient-specific geometries, namely a patient-specific sagittal and coronal curvature, as well as enhanced bone preservation. The objective of this study was to investigate the use of a novel implant design utilizing a patient specific sagittal J-curve on the femoral component combined with a novel constant, patient-derived femoral coronal curvature and to assess tibio-femoral contact area and contact stress on a femur matched curved tibial polyethylene insert. Mean contact area and standard deviations were 81+/-5, 96+/-5 and 74+/-4 mm(2) for the heel strike, toe off and mid-stance positions, respectively. Mean contact stress and standard deviations were 23.83+/-1.39, 23.27+/-1.14 and 20.78+/-0.54 MPa for the heel strike, toe off and mid-stance positions, respectively. Standard deviations of the measurements were small, not exceeding 6-7% confirming the consistency of loading conditions across different flexion angles. The results were comparable to those reported for standard, off-the-shelf fixed-bearing implants with paired femoral and tibial geometries. These data show that a constant coronal curvature can be applied to a patient-specific implant by measuring coronal curvatures across the femoral condyle in each patient and by deriving an average curvature. This novel approach combines unique benefits of patient-specific geometry with proven design concepts for minimizing polyethylene wear.
Keywords: Unicompartmental; contact stress; knee replacement.; patient specific; prosthesis design.
Figures
Similar articles
-
Influence of Preservation of Normal Knee Contact Stress on Other Compartments with respect to the Tibial Insert Design for Unicompartmental Knee Arthroplasty.Appl Bionics Biomech. 2019 Nov 14;2019:9246379. doi: 10.1155/2019/9246379. eCollection 2019. Appl Bionics Biomech. 2019. PMID: 31827605 Free PMC article.
-
[Influence of rotatory malposition of femoral implant in failure of unicompartimental medial knee prosthesis].Rev Chir Orthop Reparatrice Appar Mot. 2006 Sep;92(5):473-84. doi: 10.1016/s0035-1040(06)75834-2. Rev Chir Orthop Reparatrice Appar Mot. 2006. PMID: 17088741 French.
-
Preservation of femoral and tibial coronal alignment to improve biomechanical effects of medial unicompartment knee arthroplasty: Computational study.Biomed Mater Eng. 2018;29(5):651-664. doi: 10.3233/BME-181015. Biomed Mater Eng. 2018. PMID: 30400078
-
The unicompartmental knee: design and technical considerations in minimizing wear.Clin Orthop Relat Res. 2006 Nov;452:137-42. doi: 10.1097/01.blo.0000229358.19867.60. Clin Orthop Relat Res. 2006. PMID: 16906108 Review.
-
The conflicting requirements of laxity and conformity in total knee replacement.J Biomech. 1999 Mar;32(3):239-47. doi: 10.1016/s0021-9290(98)00139-0. J Biomech. 1999. PMID: 10093023 Review.
Cited by
-
Reduction in tibiofemoral conformity in lateral unicompartmental knee arthroplasty is more representative of normal knee kinematics.Bone Joint Res. 2020 Jan 8;8(12):593-600. doi: 10.1302/2046-3758.812.BJR-2019-0114.R1. eCollection 2019 Dec. Bone Joint Res. 2020. PMID: 31934330 Free PMC article.
-
Influence of tibiofemoral congruency design on the wear of patient-specific unicompartmental knee arthroplasty using finite element analysis.Bone Joint Res. 2019 Apr 2;8(3):156-164. doi: 10.1302/2046-3758.83.BJR-2018-0193.R1. eCollection 2019 Mar. Bone Joint Res. 2019. PMID: 30997041 Free PMC article.
-
The biomechanical effect of tibiofemoral conformity design for patient-specific cruciate retainging total knee arthroplasty using computational simulation.J Exp Orthop. 2019 Jun 3;6(1):23. doi: 10.1186/s40634-019-0192-6. J Exp Orthop. 2019. PMID: 31161463 Free PMC article.
-
Malpositioning of Prosthesis: Patient-specific Total Knee Arthroplasty Versus Standard Off-the-Shelf Total Knee Arthroplasty.J Am Acad Orthop Surg Glob Res Rev. 2017 Aug 2;1(4):e020. doi: 10.5435/JAAOSGlobal-D-17-00020. eCollection 2017 Jul. J Am Acad Orthop Surg Glob Res Rev. 2017. PMID: 30211354 Free PMC article.
-
Prediction of wear performance in femoral and tibial conformity in patient-specific cruciate-retaining total knee arthroplasty.J Orthop Surg Res. 2020 Jan 22;15(1):24. doi: 10.1186/s13018-020-1548-4. J Orthop Surg Res. 2020. PMID: 31969195 Free PMC article.
References
-
- Riddle DL, Jiranek WA, McGlynn FJ. “Yearly incidence of unicompartmental knee arthroplasty in the United States”. J. Arthroplasty. 2008 Apr;23(3):408–12. - PubMed
-
- Vince KG, Cyran LT. “Unicompartmental knee arthroplasty: new indications, more complications?”. J. Arthroplasty. 2004 Jun;19(4) Suppl 1:9–16. - PubMed
-
- Cameron HU, Jung YB. “A comparison of unicompartmental knee replacement with total knee replacement”. Orthop. Rev. 1988 Oct;17(10):983–8. - PubMed
-
- Kozinn SC, Scott R. “Unicondylar knee arthroplasty”. J. Bone Joint Surg. Am. 1989 Jan;71(1):145–50. - PubMed
-
- Furnes A, Lie SA, Havelin LI, Engesaeter LB, Vollset SE. “The economic impact of failures in total hip replacement surgery: 28,997 cases from the Norwegian Arthroplasty Register, 1987-1993”. Acta. Orthop. Scand. 1996 Apr;67(2):115–21. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous