

Randomized phase II study of gemcitabine plus radiotherapy versus gemcitabine, 5-fluorouracil, and cisplatin followed by radiotherapy and 5-fluorouracil for patients with locally advanced, potentially resectable pancreatic adenocarcinoma
- PMID: 20461765
- PMCID: PMC4403240
- DOI: 10.1002/jso.21527
Randomized phase II study of gemcitabine plus radiotherapy versus gemcitabine, 5-fluorouracil, and cisplatin followed by radiotherapy and 5-fluorouracil for patients with locally advanced, potentially resectable pancreatic adenocarcinoma
Abstract
Purpose: A randomized phase II trial (E1200) was designed to assess toxicities and surgical resection rates in two neoadjuvant gemcitabine-based chemoradiation regimens in patients with borderline resectable pancreatic cancer. The trial was terminated early due to poor accrual.
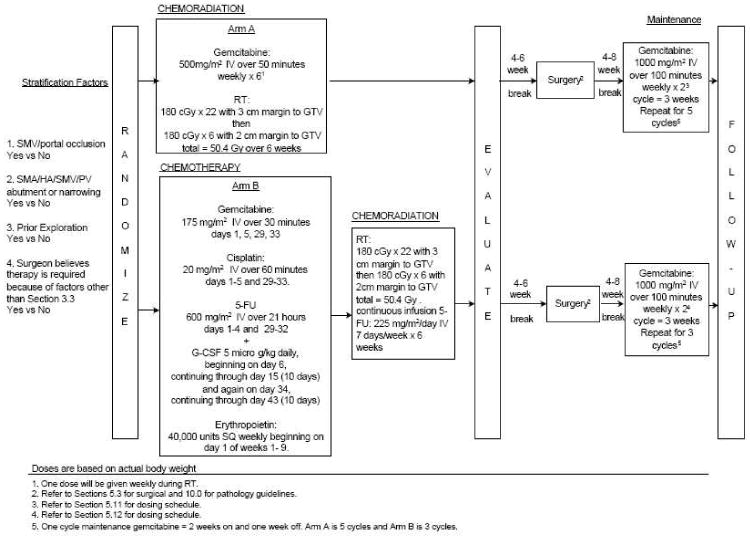
Patients and methods: Patients with borderline resectable adenocarcinomas of the pancreas were enrolled. Arm A patients (n = 10) received gemcitabine 500 mg/m(2) IV weekly for 6 weeks, with radiation to 50.4 Gy followed by surgical resection. Arm B patients (n = 11) received preoperative gemcitabine 175 mg/m(2) on days 1, 5, 29, and 33, cisplatin 20 mg/m(2) on days 1-5 and 29-32, 5-FU 600 mg/m(2) on days 1-5 and 29-32, followed by radiation with continuous infusion 5-FU 225 mg/m(2) for 6 weeks. All patients received adjuvant gemcitabine 1,000 mg/m(2) weekly x 3 for five cycles.
Results: Three patients in arm A, and two patients in arm B were resected. Hematologic toxicity was comparable between the two arms except more patients in arm B developed grade 3 or 4 thrombocytopenia than those in arm A. Arm B had fewer grade 1-2 GI toxicities although more patients (45%) experienced grade 3-4 GI toxicity.
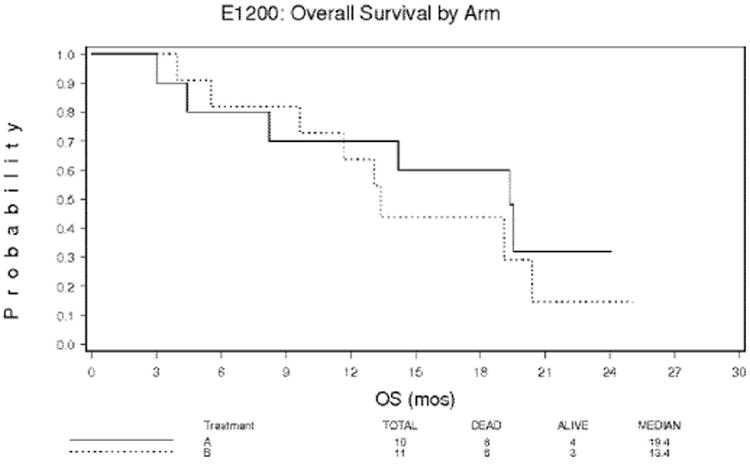
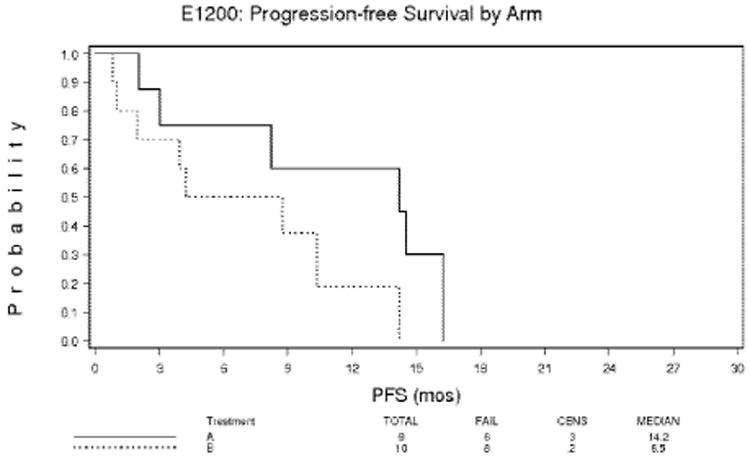
Conclusions: This phase II trial showed that both regimens were tolerable, and resectability and survival were comparable to previous studies.
Figures
References
-
- Lawrence TS, Eisbruch A, Shewach DS. Gemcitabine-mediated radiosensitization. Semin Oncol. 24(2 Suppl 7):S7-24–S7-28. 1997. - PubMed
-
- Burris HA, 3rd, Moore MJ, Anderson J, et al. Phase I and pharmacologic study of oral topotecan administered twice daily for 21 days to adult patients with solid tumors. J Clin Oncol. 15:1087–93. 1997. - PubMed
-
- Rothenberg ML, Benedetti JK, Macdonald JS, et al. Phase II trial of 5-fluorouracil plus eniluracil in patients with advanced pancreatic cancer: a Southwest Oncology Group study. Ann Oncol. 2002;13:1576–82. - PubMed
-
- Moossa AR, Lewis MH, Mackie CR. Surgical treatment of pancreatic cancer. Mayo Clinic Proceedings. 1979 Jul;54(7):468–74. - PubMed
-
- Regine WF, Winter KA, Abrams RA, et al. Flurouracil vs gemcitabine chemotherapy before and after fluorouracil-based chemoradiation following resection of pancreatic adenocarcinoma. JAMA. 2008;299:1019–1026. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- CA21076/CA/NCI NIH HHS/United States
- U10 CA027525/CA/NCI NIH HHS/United States
- CA07190/CA/NCI NIH HHS/United States
- CA66636/CA/NCI NIH HHS/United States
- U10 CA021115/CA/NCI NIH HHS/United States
- CA27525/CA/NCI NIH HHS/United States
- U10 CA017145/CA/NCI NIH HHS/United States
- U10 CA021076/CA/NCI NIH HHS/United States
- U10 CA066636/CA/NCI NIH HHS/United States
- CA17145/CA/NCI NIH HHS/United States
- CA49957/CA/NCI NIH HHS/United States
- U10 CA049957/CA/NCI NIH HHS/United States
- U10 CA023318/CA/NCI NIH HHS/United States
- U10 CA007190/CA/NCI NIH HHS/United States
- CA21115/CA/NCI NIH HHS/United States
- CA23318/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
