

MR imaging of deltoid ligament pathologic findings and associated impingement syndromes
- PMID: 20462992
- PMCID: PMC2868501
- DOI: 10.1148/rg.303095756
MR imaging of deltoid ligament pathologic findings and associated impingement syndromes
Abstract
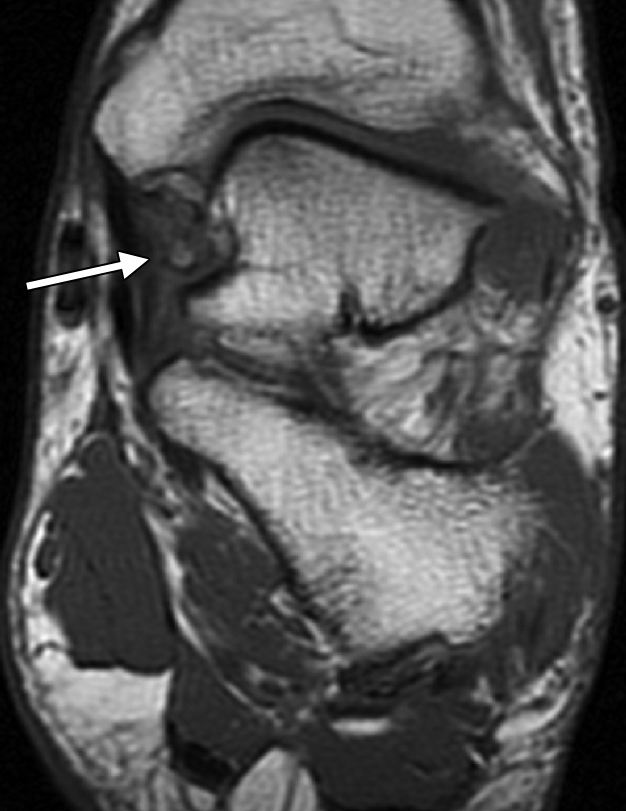
Injuries of the deltoid ligament of the ankle are increasingly recognized with the widespread use of magnetic resonance (MR) imaging. The use of higher magnetic field strengths requires familiarity with the anatomic substructure of the deltoid ligament to better localize and characterize pathologic findings. Specifically, improved image resolution allows components of the superficial (tibiocalcaneal, tibionavicular, posterior superficial tibiotalar, and tibiospring ligaments) and deep (anterior tibiotalar and posterior deep tibiotalar ligaments) portions of the ligament to be evaluated separately. Awareness of the deltoid ligament substructure and associated injury patterns can guide the radiologist in defining underlying mechanical derangement, such as that seen in various impingement disorders. In this review article, the MR imaging technique for the deltoid ligament is summarized, and the normal and abnormal MR imaging appearances of various components of the deltoid ligament and associated impingement syndromes are presented.
Figures







































References
-
- Muhle C, Frank LR, Rand T, et al. Collateral ligaments of the ankle: high-resolution MR imaging with a local gradient coil and anatomic correlation in cadavers. RadioGraphics 1999;19(3):673–683 - PubMed
-
- Stoller DW.Magnetic resonance imaging in orthopaedics and sports medicine 3rd ed.Baltimore, Md: Lippincott Williams & Wilkins, 2006; 786–793
-
- Pankovich AM, Shivaram MS.Anatomical basis of variability in injuries of the medial malleolus and the deltoid ligament. I. Anatomical studies. Acta Orthop Scand 1979;50(2):217–223 - PubMed
-
- Hintermann B.Biomechanics of the unstable ankle joint and clinical implications. Med Sci Sports Exerc 1999;31(suppl 7):S459–S469 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
