

Failure to recover to baseline pulmonary function after cystic fibrosis pulmonary exacerbation
- PMID: 20463179
- PMCID: PMC5450763
- DOI: 10.1164/rccm.200909-1421OC
Failure to recover to baseline pulmonary function after cystic fibrosis pulmonary exacerbation
Abstract
Rationale: Patients with cystic fibrosis periodically experience pulmonary exacerbations. Previous studies have noted that some patients' lung function (FEV(1)) does not improve with treatment.
Objectives: To determine the proportion of patients treated for a pulmonary exacerbation that does not recover to spirometric baseline, and to identify factors associated with the failure to recover to spirometric baseline.
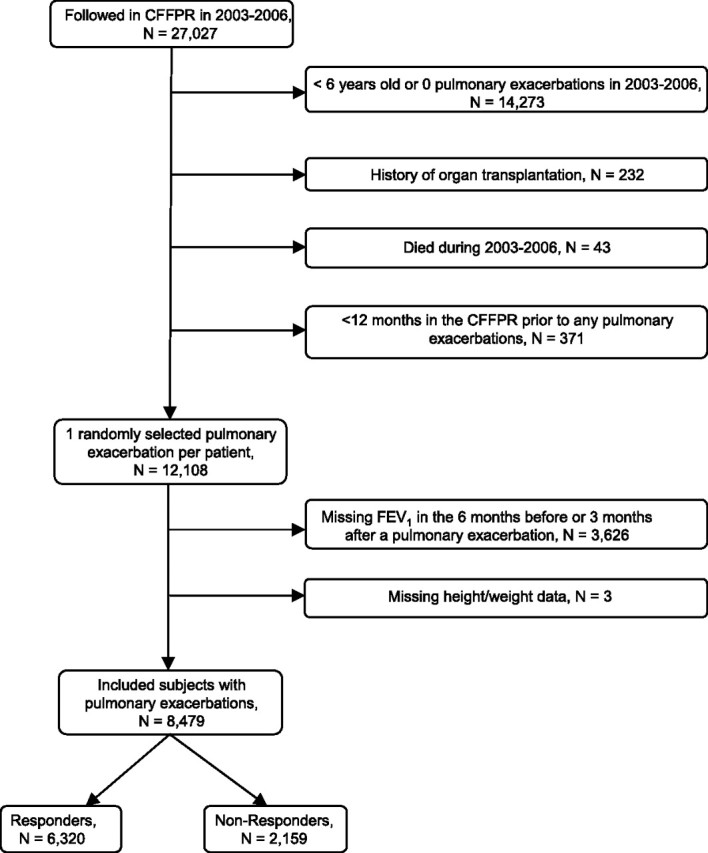
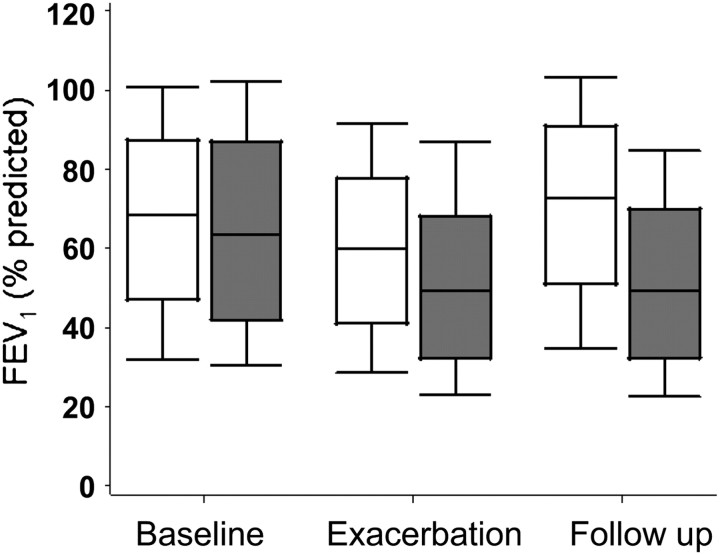
Methods: Cohort study using the Cystic Fibrosis Foundation Patient Registry from 2003-2006. We randomly selected one pulmonary exacerbation treated with intravenous antibiotics per patient and compared the best FEV(1) in the 3 months after treatment with the best FEV(1) in the 6 months before treatment. Recovery to baseline was defined as any FEV(1) in the 3 months after treatment that was greater than or equal to 90% of the baseline FEV(1). Multivariable logistic regression was used to estimate associations with the failure to recover to baseline FEV(1).
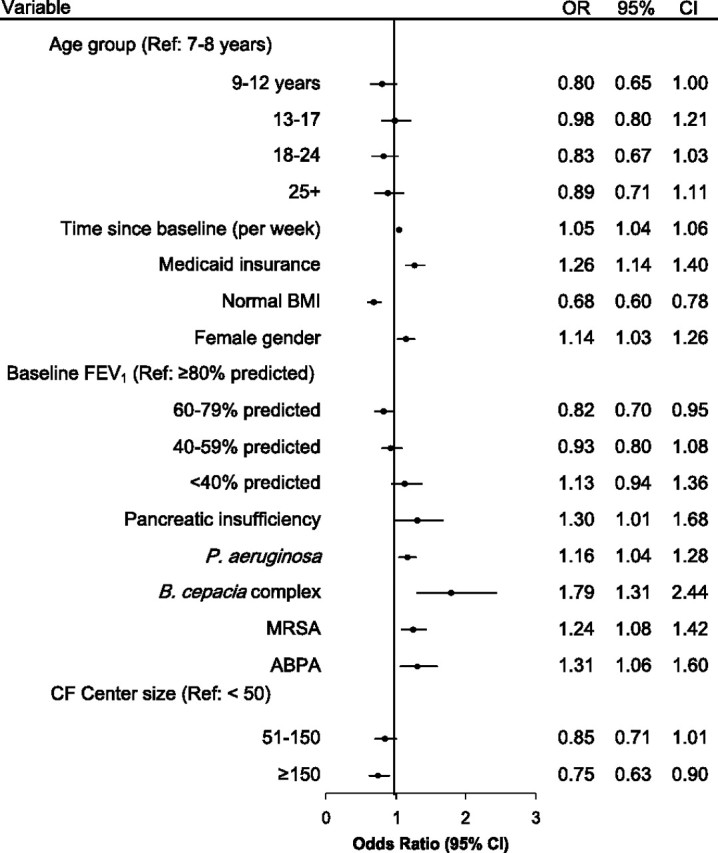
Measurements and main results: Of 8,479 pulmonary exacerbations, 25% failed to recover to baseline FEV(1). A higher risk of failing to recover to baseline was associated with female sex; pancreatic insufficiency; being undernourished; Medicaid insurance; persistent infection with Pseudomonas aeruginosa, Burkholderia cepacia complex, or methicillin-resistant Staphylococcus aureus; allergic bronchopulmonary aspergillosis; a longer time since baseline spirometric assessment; and a larger drop in FEV(1) from baseline to treatment initiation.
Conclusions: For a randomly selected pulmonary exacerbation, 25% of patients' pulmonary function did not recover to baseline after treatment with intravenous antibiotics. We identified factors associated with the failure to recover to baseline, allowing clinicians to identify patients who may benefit from closer monitoring and more aggressive treatment.
Figures
References
-
- Ramsey B. Management of pulmonary disease in patients with cystic fibrosis. N Engl J Med 1996;335:179–188. - PubMed
-
- Ferkol T, Rosenfeld M, Milla CE. Cystic fibrosis pulmonary exacerbations. J Pediatr 2006;148:259–264. - PubMed
-
- Mayer-Hamblett N, Rosenfeld M, Emerson J, Goss C, Aitken M. Developing cystic fibrosis lung transplant referral criteria using predictors of 2-year mortality. Am J Respir Crit Care Med 2002;166:1550–1555. - PubMed
-
- Lieu T, Ray G, Farmer G, Shay G. The cost of medical care for patients with cystic fibrosis in a health maintenance organization. Pediatrics 1999;103:e72. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
