

Regional variations in diagnostic practices
- PMID: 20463332
- PMCID: PMC2924574
- DOI: 10.1056/NEJMsa0910881
Regional variations in diagnostic practices
Erratum in
- N Engl J Med. 2010 Jul 8;363(2):198
Abstract
Background: Current methods of risk adjustment rely on diagnoses recorded in clinical and administrative records. Differences among providers in diagnostic practices could lead to bias.
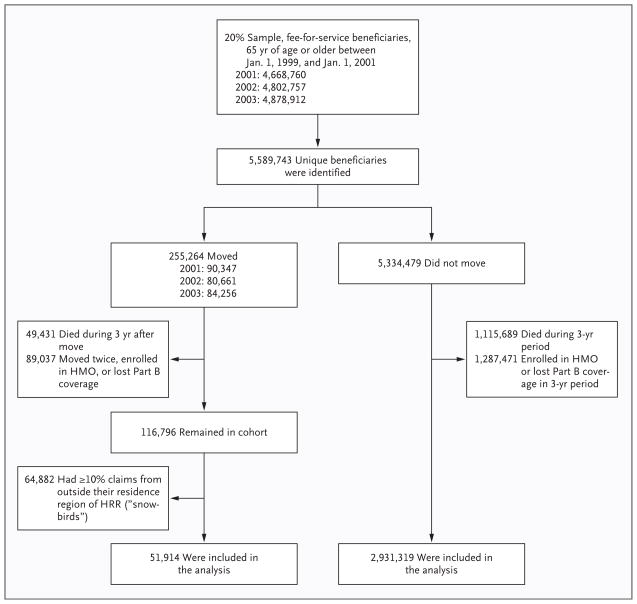
Methods: We used Medicare claims data from 1999 through 2006 to measure trends in diagnostic practices for Medicare beneficiaries. Regions were grouped into five quintiles according to the intensity of hospital and physician services that beneficiaries in the region received. We compared trends with respect to diagnoses, laboratory testing, imaging, and the assignment of Hierarchical Condition Categories (HCCs) among beneficiaries who moved to regions with a higher or lower intensity of practice.
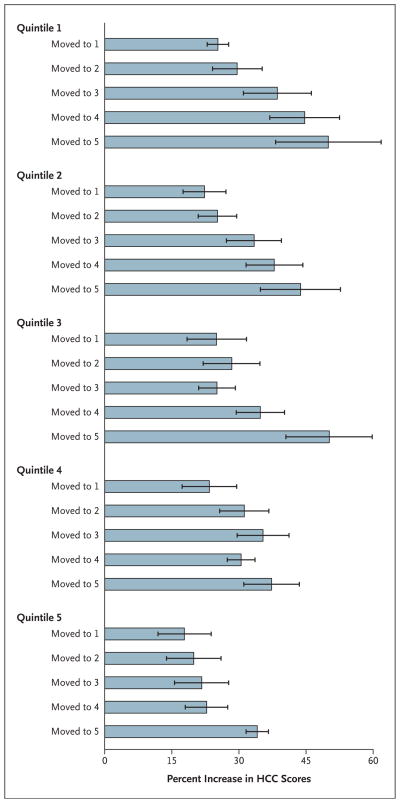
Results: Beneficiaries within each quintile who moved during the study period to regions with a higher or lower intensity of practice had similar numbers of diagnoses and similar HCC risk scores (as derived from HCC coding algorithms) before their move. The number of diagnoses and the HCC measures increased as the cohort aged, but they increased to a greater extent among beneficiaries who moved to regions with a higher intensity of practice than among those who moved to regions with the same or lower intensity of practice. For example, among beneficiaries who lived initially in regions in the lowest quintile, there was a greater increase in the average number of diagnoses among those who moved to regions in a higher quintile than among those who moved to regions within the lowest quintile (increase of 100.8%; 95% confidence interval [CI], 89.6 to 112.1; vs. increase of 61.7%; 95% CI, 55.8 to 67.4). Moving to each higher quintile of intensity was associated with an additional 5.9% increase (95% CI, 5.2 to 6.7) in HCC scores, and results were similar with respect to laboratory testing and imaging.
Conclusions: Substantial differences in diagnostic practices that are unlikely to be related to patient characteristics are observed across U.S. regions. The use of clinical or claims-based diagnoses in risk adjustment may introduce important biases in comparative-effectiveness studies, public reporting, and payment reforms.
2010 Massachusetts Medical Society
Figures
Comment in
-
Geographic variation in Medicare spending.N Engl J Med. 2010 Jul 1;363(1):85-6. doi: 10.1056/NEJMe1005212. Epub 2010 May 12. N Engl J Med. 2010. PMID: 20463335 No abstract available.
References
-
- Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, Wennberg DE, Lucas FL. Surgeon volume and operative mortality in the United States. N Engl J Med. 2003;349:2117–27. - PubMed
-
- Medicare payment basics: hospital acute inpatient services payment system. Washington, DC: Medicare Payment Advisory Commission; 2008.
-
- Skilled nursing facilities prospective payment system: overview. Baltimore: Centers for Medicare and Medicaid Services; 2009. [Accessed May 7, 2010]. at http://www.cms.hhs.gov/SNFPPS/01overview.asp.
-
- Fisher ES. Paying for performance — risks and recommendations. N Engl J Med. 2006;355:1845–7. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical