

Pregnancy and thyroid cancer: ultrasound study of foetal thyroid
- PMID: 20463840
- PMCID: PMC2868207
Pregnancy and thyroid cancer: ultrasound study of foetal thyroid
Abstract
Thyroid cancer is the most common endocrine malignancy, more frequently diagnosed in young women during childbearing age and approximately 10% of all thyroid cancers are diagnosed during pregnancy or in the early post-partum period. Thyroid cancer in young people has generally an excellent prognosis, and survival among women with thyroid cancer diagnosed during pregnancy may not differ from that in age-matched non-pregnant women with similar cancer. Pregnancy after treatment of thyroid carcinoma requires both maternal and foetal controls. Of utmost importance is to ensure adequate maintenance of maternal levels of levothyroxine, needed by both the foetal central nervous system for its normal maturation and the mother to avoid possible recurrence or spread of the disease. In the present investigation, to confirm normal foetal growth and foetal thyroid development, an ultrasound study of the foetal thyroid was performed in 40 full term pregnancies in 32 women receiving levothyroxine treatment for previously treated thyroid cancer. In patients undergoing either suppressive or substitutive levothyroxine treatment, foetal thyroid growth was noted to be normal in all the cases, newborn thyroid status was always normal, and the incidence of maternal morbidity was not influenced. In the present study group, pregnancy does not appear to compromise mother's disease-free interval, nor to be compromised by thyroid cancer treatment. Results of the present study confirm that regular adjustment of levothyroxine treatment is of utmost importance for both maternal and foetal well-being and that foetal thyroid ultrasound study may add useful and reassuring data about child well-being.
Il carcinoma della tiroide è la neoplasia endocrina più frequente, si presenta spesso in donne in età fertile, per questo motivo il 10% di tutti i carcinomi tiroidei viene diagnosticato durante la gravidanza o immediatamente dopo. I carcinomi tiroidei nei giovani presentano una prognosi eccellente e la sopravvivenza libera da malattia nelle donne cui viene diagnosticato durante la gravidanza non sembra differente da quella di pazienti non gravide con la stessa età e la stessa estensione di malattia, ma ovviamente la gravidanza dopo terapia per carcinoma tiroideo necessita un controllo duplice, sia per la madre che per il feto. Mantenere adeguati livelli di levotiroxina è di estrema importanza sia per la maturazione fetale, in particolare del sistema nervoso centrale, sia per proteggere la madre da possibili recidive di malattia. Le preoccupazioni maggiori riguardano gli effetti sul feto della terapia TSH-soppressiva e della terapia radio metabolica con I-131. Per confermare la sicurezza delle terapie sono state studiate anche con valutazione ecografica le tiroidi fetali in 40 gravidanze di 32 pazienti trattate con levotiroxina dopo chirurgia per carcinoma tiroideo. Sia per le pazienti sottoposte a terapia sostitutiva che per quelle in terapia TSH soppressiva lo studio ecografico della tiroide fetale si mostrò entro le curve di normalità. Per le pazienti di questo studio la gravidanza non sembra compromettere l’intervallo libero da malattia né essere compromessa dalle terapie utilizzate per il pregresso carcinoma tiroideo. Si conferma in questo studio che un regolare adeguamento della terapia con levotiroxina è di estrema importanza, e che lo studio ecografico della tiroide fetale può aggiungere informazioni rassicuranti sul benessere fetale.
Keywords: Foetal thyroid; Pregnancy; Thyroid cancer; Ultrasound.
Figures
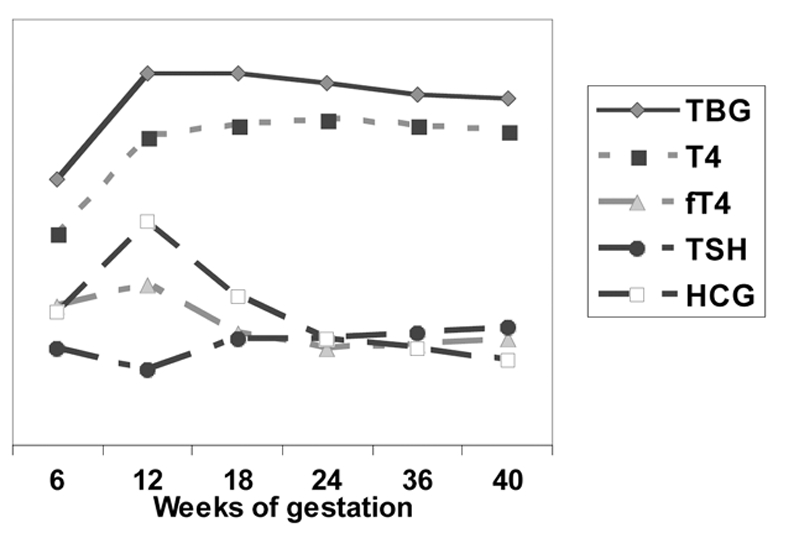
TBG (thyroxin binding globulin) increases due to stimulation from placental E2 and E3 (oestradiol and oestriol) and to reduced hepatic clearance. On account of this, maternal total T4 is very high, but fT4 is only moderately elevated.
HCG (human chorionic gonadotrophin) has thyrotropin-like activity and stimulates total T4 secretion.
TSH may decrease between week 8 to 14 of gestation, inhibited by increased T4



Similar articles
-
Management and follow-up of thyroid cancer in pregnant women.Acta Otorhinolaryngol Ital. 2011 Dec;31(6):358-65. Acta Otorhinolaryngol Ital. 2011. PMID: 22323846 Free PMC article. Review.
-
Increased size and vascularisation, plus decreased echogenicity, of foetal thyroid in two-dimensional ultrasonography caused by maternal Graves' disease.Endokrynol Pol. 2014;65(1):64-8. doi: 10.5603/EP.2014.0009. Endokrynol Pol. 2014. PMID: 24549604
-
[The fetal adrenal gland in risk pregnancy].Srp Arh Celok Lek. 2002 May-Jun;130(5-6):198-200. doi: 10.2298/sarh0206198l. Srp Arh Celok Lek. 2002. PMID: 12395443 Serbian.
-
The development of the foetal thyroid: in utero ultrasonographic measurements.Clin Endocrinol (Oxf). 1998 Mar;48(3):259-64. doi: 10.1046/j.1365-2265.1998.00388.x. Clin Endocrinol (Oxf). 1998. PMID: 9578813
-
Foetal and neonatal thyroid disorders.Minerva Pediatr. 2002 Oct;54(5):383-400. Minerva Pediatr. 2002. PMID: 12244277 Review. English, Italian.
Cited by
-
Lobectomy may be more appropriate for patients with early-stage medullary thyroid cancer older than 60 years old.Front Endocrinol (Lausanne). 2022 Oct 21;13:1015319. doi: 10.3389/fendo.2022.1015319. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36339396 Free PMC article.
-
Management and follow-up of thyroid cancer in pregnant women.Acta Otorhinolaryngol Ital. 2011 Dec;31(6):358-65. Acta Otorhinolaryngol Ital. 2011. PMID: 22323846 Free PMC article. Review.
-
Recommendations of the AGG (Working Group for Obstetrics, Department of Maternal Diseases) on How to Treat Thyroid Function Disorders in Pregnancy.Geburtshilfe Frauenheilkd. 2023 Mar 9;83(5):504-516. doi: 10.1055/a-1967-1653. eCollection 2023 May. Geburtshilfe Frauenheilkd. 2023. PMID: 37152543 Free PMC article.
-
Investigation of 7-dehydrocholesterol reductase pathway to elucidate off-target prenatal effects of pharmaceuticals: a systematic review.Pharmacogenomics J. 2016 Oct;16(5):411-29. doi: 10.1038/tpj.2016.48. Epub 2016 Jul 12. Pharmacogenomics J. 2016. PMID: 27401223 Free PMC article.
References
-
- Alexander EK, Marqusee E, Lawrence J, Jarolim P, Fisher GA, Larsen PR. Timing and magnitude of increases in levothyroxine requirements during pregnancy in women with hypothyroidism. N Engl J Med 2004;351:241-9. - PubMed
-
- Glinoer D. Management of hypo- and hyperthyroidism during pregnancy. Growth Hormone & Igf Research 2003;13(Suppl A):S45-S54. - PubMed
-
- Lao TT. Thyroid disorders in pregnancy. Curr Opin Obstet Gynecol 2005;17:123-7. - PubMed
-
- Lazarus JH. Thyroid disorders associated with pregnancy etiology, diagnosis and management. Treat Endocrinol 2005;4:31-41. - PubMed
-
- Obregon MJ, Calvo RM, Escobar del Rey F, Morreale de Escobar G. Thyroid hormones and foetal developmernt. In: Pinchera A, Mann K, Hostalec U, editors. The thyroid and age. Stuttgart: Schattauer Verlagsgesellschaft mbH; 1998. p. 49-73.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical