

Wireless pH-motility capsule for colonic transit: prospective comparison with radiopaque markers in chronic constipation
- PMID: 20465593
- PMCID: PMC2911492
- DOI: 10.1111/j.1365-2982.2010.01517.x
Wireless pH-motility capsule for colonic transit: prospective comparison with radiopaque markers in chronic constipation
Abstract
Background: Colon transit (CT) measurements are used in the management of significant constipation. The radiopaque marker (ROM) method provides limited information.
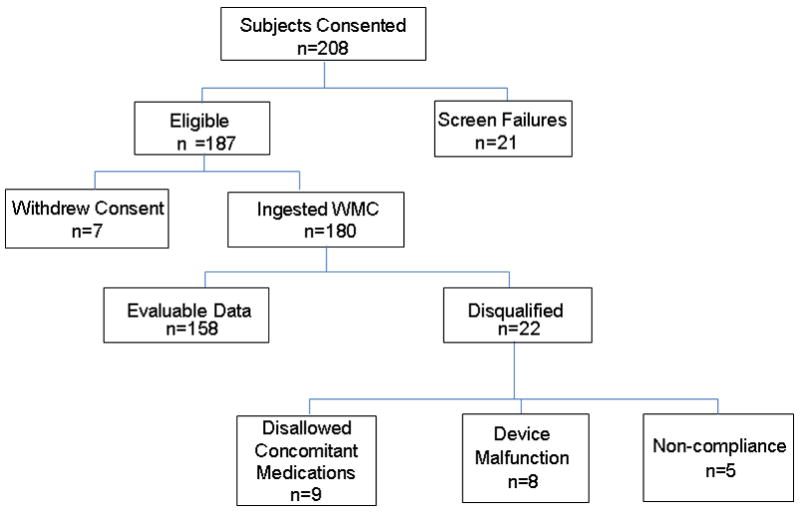
Methods: We proposed to validate wireless motility capsule (WMC), that measures pH, pressure and temperature, to ROM measurement of CT in patients with symptomatic constipation evaluated at multiple centers. Of 208 patients recruited, 158 eligible patients underwent simultaneous measurement of colonic transit time (CTT) using ROM (Metcalf method, cut off for delay >67 h), and WMC (cutoff for delay >59 h). The study was designed to demonstrate substantial equivalence, defined as diagnostic agreement >65% for patients who had normal or delayed ROM transit.
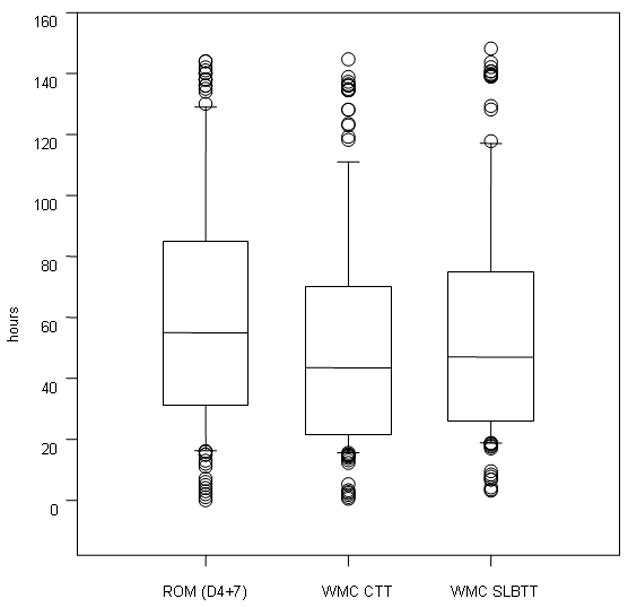
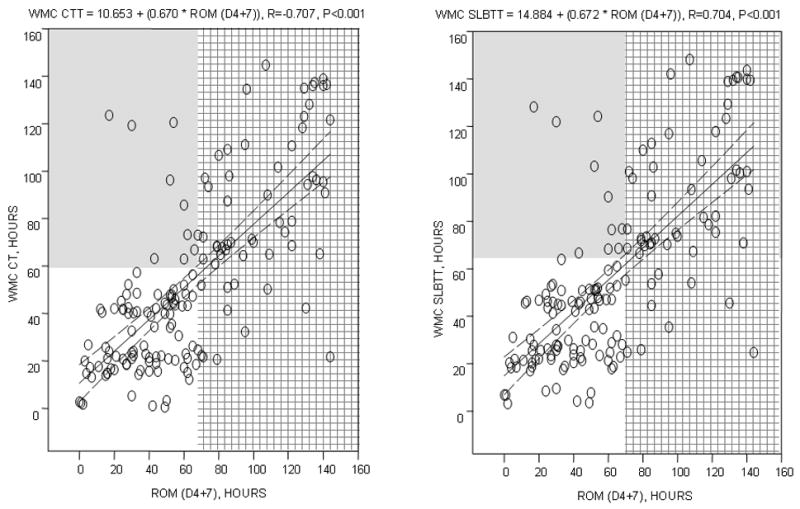
Key results: Fifty-nine of 157 patients had delayed ROM CT. Transit results by the two methods differed: ROM median 55.0 h [IQR 31.0-85.0] and WMC (43.5 h [21.7-70.3], P < 0.001. The positive percent agreement between WMC and ROM for delayed transit was approximately 80%; positive agreement in 47 by WMC/59 by ROM or 0.796 (95% CI = 0.67-0.98); agreement vs null hypothesis (65%) P = 0.01. The negative percent agreement (normal transit) was approximately 91%: 89 by WMC/98 by ROM or 0.908 (95% CI = 0.83-0.96); agreement vs null hypothesis (65%), P = 0.00001. Overall device agreement was 87%. There were significant correlations (P < 0.001) between ROM and WMC transit (CTT [r = 0.707] and between ROM and combined small and large bowel transit [r = 0.704]). There were no significant adverse events.
Conclusions & inferences: The 87% overall agreement (positive and negative) validates WMC relative to ROM in differentiating slow vs normal CT in a multicenter clinical study of constipation.
Trial registration: ClinicalTrials.gov NCT00857363.
Conflict of interest statement
Dr. Rao, Dr. Hasler, Dr. Kuo, Dr. McCallum, Dr. Parkman, Dr. Scott, Dr. Wilding serve as speakers, consultants, or advisory board members for the SmartPill Corporation. These authors and Dr. Soffer have received research funding for other research studies from the SmartPill Corporation.
Dr. Semler is an employee of the SmartPill Corporation and owns stock in the SmartPill Corporation.
Figures
References
-
- Higgins DR, Johanson JF. Epidemiology of constipation in North America: a systematic review. Am J Gastroenterol. 2004;99:750–759. - PubMed
-
- Lembo A, Camilleri M. Chronic constipation. N Engl J Med. 2003;349:1360–1368. - PubMed
-
- Rao SS, Ozturk R, Laine L. Clinical utility of diagnostic tests for constipation in adults: a systematic review. Am J Gastroenterol. 2005;100:1605–1615. - PubMed
-
-
Rome III [The Rome Foundationhttp://www.romecriteria.org/questionnaires ])
-
-
- Brandt LJ, Prather CM, Eamonn MM, et al. Systematic review on the management of chronic constipation in North America. Am J Gastroenerol. 2005;100(S1):S5–S21. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
