

Chronic coccidioidomycosis endophthalmitis without concomitant systemic involvement: a clinicopathological case report
- PMID: 20471688
- PMCID: PMC2933969
- DOI: 10.1016/j.ophtha.2010.01.033
Chronic coccidioidomycosis endophthalmitis without concomitant systemic involvement: a clinicopathological case report
Abstract
Objective: To report the diagnostic, clinical, and histopathologic features of a patient with coccidioidomycosis endophthalmitis without concomitant systemic involvement diagnosed by vitreous biopsy.
Design: Interventional case report.
Participants: One patient.
Intervention: Diagnostic pars plana vitrectomy, systemic and intravitreal antifungal treatment, and enucleation.
Main outcome measures: Diagnostic, clinical, and histopathologic features of chronic coccidioidomycosis endophthalmitis.
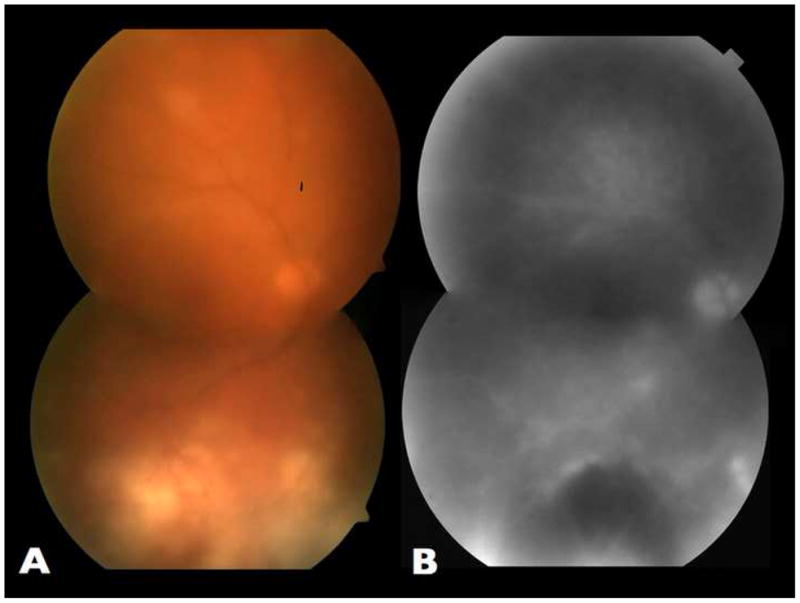
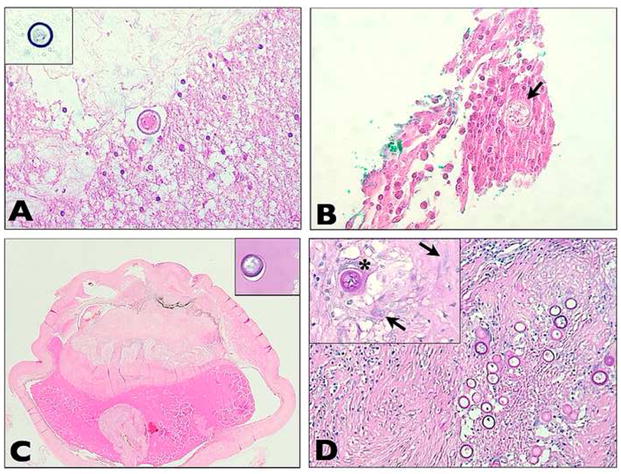
Results: A 64-year-old white man from Southern California presented with chronic intraocular inflammation in the right eye that had lasted 18 months. He had been unsuccessfully treated with topical and subtenon steroids. At presentation, best-corrected visual acuity was 20/400 in the right eye and 20/20 in the left eye. Ophthalmoscopy of the right eye revealed significant vitritis and multiple yellowish chorioretinal lesions. Evaluation by an internist showed no underlying inflammatory, infectious, or neoplastic systemic illnesses. A vitreous biopsy followed by histopathologic examination showed the presence of multiple Coccidioides sp. microorganisms. The patient was then treated with intravitreal amphotericin B and oral fluconazole. Best-corrected visual acuity initially improved to 20/80, but inflammation progressed and did not respond to 2 subsequent injections of antifungals, 2 additional pars plana vitrectomies, and oral fluconazole. The eye eventually became blind and painful and was enucleated. Histopathologic examination disclosed intraocular granulomas displaying multiple Coccidioides sp. microorganisms.
Conclusions: Coccidioides sp. endophthalmitis may present with no concomitant systemic involvement. Histopathologic examination of the vitreous is helpful in the diagnosis. A high index of suspicion is important, especially in areas where the incidence of coccidioidomycosis is rising.
Copyright © 2010 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
There is no conflict of interest for any author.
Figures
References
-
- Chiller TM, Galgiani JN, Stevens DA. Coccidioidomycosis. Infect Dis Clin North Am. 2003;17:41–57. viii. - PubMed
-
- Ampel NM. Coccidioidomycosis: a review of recent advances. Clin Chest Med. 2009;30:241–51. v. - PubMed
-
- Rodenbiker HT, Ganley JP. Ocular coccidioidomycosis. Surv Ophthalmol. 1980;24:263–90. - PubMed
-
- Foos RY, Zakka KA. Coccidioidomycosis. In: Pepose JS, Holland GN, Wilhelmus KR, editors. Ocular Infection and Immunity. St. Louis, MO: Mosby; 1996. pp. 1430–6.
-
- Increase in coccidioidomycosis - California, 2000–2007. MMWR Morb Mortal Wkly Rep. 2009;58:105–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
