

Shoulder function and anatomy in complete obstetric brachial plexus palsy: long-term improvement after triangle tilt surgery
- PMID: 20473676
- PMCID: PMC2903705
- DOI: 10.1007/s00381-010-1174-2
Shoulder function and anatomy in complete obstetric brachial plexus palsy: long-term improvement after triangle tilt surgery
Abstract
Purpose: Untreated complete obstetric brachial plexus injury (COBPI) usually results in limited spontaneous recovery of shoulder function. Older methods used to treat COBPI have had questionable success, with very few studies being published. The purpose of the current study was to examine the results of triangle tilt surgery on shoulder function and development in COBPI individuals.
Methods: This study was conducted as a retrospective chart review. Inclusion criteria were COBPI patients that had undergone the triangle tilt procedure from 2005 to 2009 and were between the ages of 9 months and 12 years. COBPI was defined as permanent injury to all five nerve roots (C5-T1), with significant degradation in development and function of the hand. Twenty-five patients with a mean age of 5 (0.75-12) years were followed up clinically for more than 2 years.
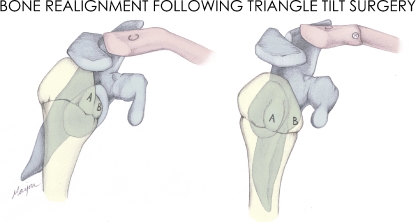
Results: The triangle tilt procedure resulted in demonstrable clinical enhancements with appreciable improvements in shoulder function, glenoid version, and humeral head congruity. There was a significant increase in the overall Mallet score (2.4 points, p < 0.0001) following surgical correction in patients that were followed up for more than 2 years.
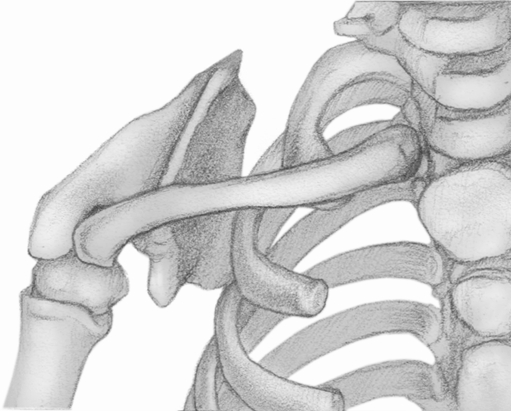
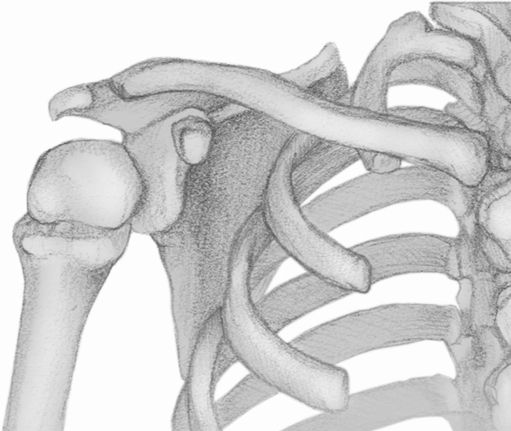
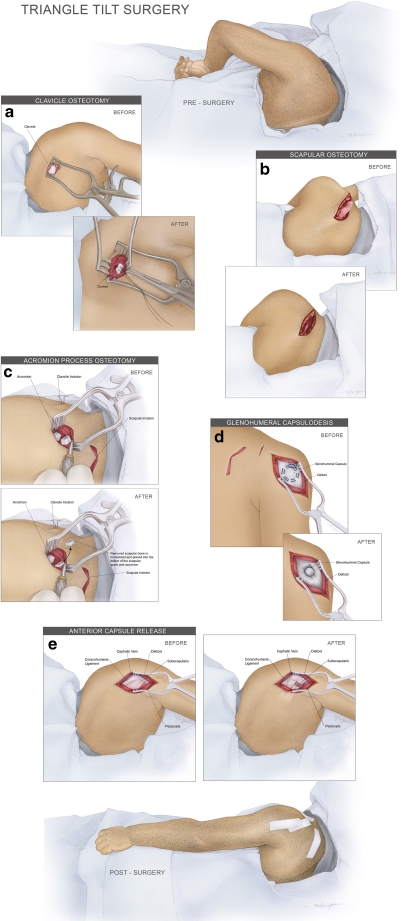
Conclusions: The results of this study demonstrate that COBPI patients who develop SHEAR and medial rotation contracture deformities can benefit from the triangle tilt surgery, which improves shoulder function and anatomy across a range of pediatric ages. Despite these patients presenting late for surgery in general (5 years), significant improvements were observed in their glenohumeral (GH) dysplasia and their ability to perform shoulder and arm movements following surgery.
Figures

Similar articles
-
Long-term outcomes of triangle tilt surgery for obstetric brachial plexus injury.Pediatr Surg Int. 2010 Apr;26(4):393-9. doi: 10.1007/s00383-010-2550-4. Epub 2010 Feb 4. Pediatr Surg Int. 2010. PMID: 20130887 Free PMC article.
-
Triangle tilt surgery as salvage procedure for failed shoulder surgery in obstetric brachial plexus injury.Pediatr Surg Int. 2010 Sep;26(9):913-8. doi: 10.1007/s00383-010-2673-7. Epub 2010 Jul 29. Pediatr Surg Int. 2010. PMID: 20668864 Free PMC article.
-
Effect of tendon transfers and extra-articular soft-tissue balancing on glenohumeral development in brachial plexus birth palsy.J Bone Joint Surg Am. 2005 Feb;87(2):320-5. doi: 10.2106/JBJS.C.01614. J Bone Joint Surg Am. 2005. PMID: 15687154
-
Arthroscopic treatment for internal contracture of the shoulder secondary to brachial plexus birth palsy: report of a case series and review of the literature.Eur J Orthop Surg Traumatol. 2015 Oct;25(7):1121-9. doi: 10.1007/s00590-015-1670-x. Epub 2015 Jul 14. Eur J Orthop Surg Traumatol. 2015. PMID: 26169993 Review.
-
Improving shoulder and elbow function in children with Erb's palsy.Semin Pediatr Neurol. 2000 Mar;7(1):44-51. doi: 10.1016/s1071-9091(00)80009-1. Semin Pediatr Neurol. 2000. PMID: 10749513 Review.
Cited by
-
Peripheral nerve injuries in the pediatric population: a review of the literature. Part I: traumatic nerve injuries.Childs Nerv Syst. 2019 Jan;35(1):29-35. doi: 10.1007/s00381-018-3974-8. Epub 2018 Sep 13. Childs Nerv Syst. 2019. PMID: 30215119
-
Comparing functional outcome of triangle tilt surgery performed before versus after two years of age.Open Orthop J. 2011 Mar 16;5:59-62. doi: 10.2174/1874325001105010059. Open Orthop J. 2011. PMID: 21566737 Free PMC article.
-
Triangle tilt and steel osteotomy: similar approaches to common problems.Open Orthop J. 2011 Mar 24;5:124-33. doi: 10.2174/1874325001105010124. Open Orthop J. 2011. PMID: 21584207 Free PMC article.
-
Outcomes of Brachial Plexus Neurolysis in 40 Patients With Obstetric Brachial Plexus Injury.Eplasty. 2025 Jan 29;25:e4. eCollection 2025. Eplasty. 2025. PMID: 40469489 Free PMC article.
-
Kinesio arm taping as prophylaxis against the development of Erb's Engram.J Adv Res. 2013 Nov;4(6):485-91. doi: 10.1016/j.jare.2012.08.006. Epub 2012 Oct 1. J Adv Res. 2013. PMID: 25685456 Free PMC article.
References
-
- Hoeksma AF, Ter Steeg AM, Dijkstra P, Nelissen RG, Beelen A, de Jong BA. Shoulder contracture and osseous deformity in obstetrical brachial plexus injuries. J Bone Joint Surg (Am) 2003;85-A:316–322. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
